He was just about my age, but his face was pale, his cheeks cavernous, and there was a weariness in his every movement; he was too weak to speak or even swallow well. It was as if he had been drained of all his youth.
We spent the next three hours helping him get through a bowl of porridge, and I will forever remember it. He struggled with every spoonful, and watching that made me sad and angry at life for being so unfair to someone as young as him. There was also an odd sense of relief whenever he did not choke on a swallow, warmth whenever he mustered enough energy to smile at me, and the type of calm you feel when you watch the ocean waves. But instead, I was watching his bony ribcage heave up and down with every breath.
That was the first day of my first job as a teenager, as a carer at St Joseph’s Hospice and Home in Singapore. I continued that job for four years and it inspired me to attend medical school. More importantly, however, those three hours were when I first discovered hospice and palliative care. Or rather, when it discovered me.
Since then, an aging population has become a major demographic trend worldwide and the topic of how to die well has garnered growing attention. Moreover, much focus has been directed to removing the taboo on death, a significant hurdle to the routine integration of palliative care into medicine [1]. As a fourth year medical student now, some deaths have inevitably left their marks on me, leading me to consider whether the palliative care we are offering to patients now really is the best. After all, in death, as in life, quality matters.
One of these deaths was that of a patient, Maggie[1], to whom I had provided care for a long time at St Joseph’s. Maggie was a retired dance teacher. She was chatty and had always proudly shared the stories of her students with me. Even after I left Singapore to attend medical school in Sydney, I would visit her whenever I made a trip back home. Unfortunately, with each visit she grew frailer, and she was eventually placed in a wheelchair, where she was spent most of her time. Her frailty took away much of her independence, but she remained cheerful, nonetheless.
At this time, St Joseph’s had begun working with a Singaporean philanthropic house, Lien Foundation, which conceptualised and pioneered the “Happy Coffin” palliative movement. The antithesis in the name of the movement captures its objective – to transform the coffin from a negative representation of death to a canvas for positive celebrations of life and expression of art. It is part of an initiative to lift the death taboo, encouraging hospice patients to share their lives, dreams, and wishes, which are interpreted and painted on a custom coffin by commissioned artists to liberate mind sets and open the “die-logue” [2]. Maggie was thus enrolled with Happy Coffin.
On my last visit to see Maggie, she showed me pictures of her coffin and described the drawings on them with a bright smile on her face. She said the lively children painted on it – her students – were the pride of her life. She seemed at peace with her condition and I felt genuinely happy for her. This seemed to reinforce what medical school had been teaching me: talking and planning for your death through palliative care really is the gold standard of dying.
A year later, I received news that Maggie has passed on. As one of the pioneer participants of the Happy Coffin experience, her death was highly publicised in the media, where she was positioned as the brave individual who confronted death optimistically, almost as the role model for all future deaths. Indeed, the moral strength of character of a patient who faces up to or denies death is always at stake whenever telling the story of death, and perhaps this is why we are fixated with open discussion of death and palliative integration [3]. They say she had a beautiful death.
However, the news of Maggie’s passing arrived in my first clinical year of medicine, during my oncology placement, a time where I was becoming increasingly aware that not every death is – or can be like Maggie’s.
There were many deaths in oncology, and thus many opportunities for palliative medicine to step in. While there were cases where palliation was seamlessly introduced into the care of terminally ill patients, I also witnessed many instances where palliative care implementation brought much distress and dilemmas in terms of medication choice, truth-telling, autonomy, and other treatment practises. Unlike what I had imagined, many patients were offended whenever death and palliation were mentioned, as some cultures believe that to speak of death is to invite it. In terms of pain management, different patients also had very different attitudes. Most doctors I met genuinely believed that pain relief is always the best option, although this can be quite controversial as many ethnic groups view pain tolerance as a form of strength. I particularly recall a Buddhist patient with staunch Confucian beliefs. Decision-making for his treatment was relinquished to his children, whose filial piety was, in turn, measured by their perseverance, both financially and emotionally, through curative therapies for their sick parent, even when efforts are futile. Such perseverance was a form of devotion and love. Palliation for this patient was, therefore, almost out of the question. On another occasion, I also observed a family get upset when the doctor had suggested for advanced care directives to be established – they saw it as prolonging autonomy when autonomy was not sought.
This set me thinking about the current model of palliation in medicine.
In medicine, we believe palliative medicine is the gold standard for dying, with the 2014 World Health Assembly prioritising the assimilation of palliative care and death planning into national healthcare systems [4]. The surge in this global palliative movement is understandably so, as palliation offers awareness and open communication, gradual acceptance of death, provision of pain relief, and continuity of a person’s essence till death in the form of autonomy in decision-making and control in the dying process. Patients who have been palliated thus approach end-of-life with symptomatic pharmacological care, spiritual, and psychosocial relief to them and their family, abundant knowledge of their disease’s natural history to manage expectations, and having their resuscitation status, medical proxies and advanced care directives established. Above all, confronting mortality empowers people to make the most of their time left, view life in wider perspectives, and live life it to the fullest [5].
However, amidst today’s palliative hype, I wonder if the medical community may have created a singular definition of a “good death”, forgetting that this definition may vary for different patients. Maggie’s death was the first death I had encountered in a healthcare setting, and I had the privilege of understanding her and her palliation process; death was openly discussed with her, she had her advanced care directives prepared, curative therapies were stopped in place of symptomatic ones, and as a Catholic, she was attending weekly prayer support sessions from the church associated with the hospice. I saw how comfortable she was even in her last months, and I am convinced that this was the best possible death for her. However, is this enough reason for deaths like hers to be touted as the role model for all other deaths, especially in today’s multicultural societies?
As our world becomes increasingly globalised and culturally diverse, our definitions of a “good” death will also diversify. This will inadvertently lead to provision of inappropriate end-of-life care to patients from diverse backgrounds and cultural misunderstandings. For example, a doctor’s concept of a “good” death, which is likely to be influenced by their culture as well as their personal and professional experiences, may conflict with the desires of the patient [6].
In Australia, while we are a multi-cultural society, our ethical paradigm remains firmly rooted in Western philosophical traditions. This becomes apparent when examining the medical school curriculum- the dominant paradigm through which ethics is being taught is the Western bioethical framework. Medical students are taught to keep diagnoses confidential to the patient only, and to prolong patient autonomy as much as possible. Although, doctors may reflect the diverse cultural demographics of Australia, they are educated to uphold the Western set of ethical principles even whilst caring for patients from diverse cultural backgrounds [6]. Such education might have unintentionally created a culture of marginalising other modes of death in the pursuit of what we were taught is a “good” death.
Perhaps more flexibility in models of end-of-life care might allow us as a medical community to better accommodate the care preferences of people from diverse backgrounds. This can be achieved through a wider appreciation of different cultural notions of death. While it is not realistic for health professionals to understand the breadth of cultural beliefs in relation to illness, it is necessary to have a fundamental level of cultural competence and to understand when, and how, to consult further expertise when caring for people of different backgrounds.
It is as much the professional responsibility of the doctor as it is the moral responsibility of friends and family to ensure that a patient’s death is in line with his/her wishes. Therefore, it really is time to open up this “die-logue” and examine how the different ideals of death seep through our current framework of palliative medicine, to decrease disparity in quality of death delivered to everyone. And who better to lead this “die-logue” than the medical community itself?
Conflicts of interest
None declared.
References
[1] Gardner DB. Quality in life and death: can we have the conversations? Nurs Econ. 2012;30(4):224.
[2] Lee PW. A Happy Coffin before you die. Singapore: Lien Foundation; 2011.
[3] Frith H, Raisborough J, Klein O. Making death ‘good’: instructional tales for dying in newspaper accounts of Jade Goody’s death. Sociol. Health Illn. 2013;35(3):419-33.
[4] Unit EI. The quality of death: ranking end of life care across the world. London: Economist Intelligence Unit; 2011.
[5] Sepúlveda C, Marlin A, Yoshida T, Ullrich A. Palliative care: the World Health Organization’s global perspective. J Pain Symptom Manage. 2002;24(2):91-6.
[6] Chater K, Tsai CT. Palliative care in a multicultural society: a challenge for western ethics. Aust J Adv Nurs. 2008;26(2):95.
A multitude of changes are revolutionising the study and practice of oncology worldwide. Despite the undeniable importance of cancer education, there is currently no consensus amongst Australian medical schools as to what should be taught regarding oncology practice, nor have the best ways of teaching and learning about cancer been fully elucidated in the literature, or in the clinical realm. There is a lack of important cancer knowledge amongst graduating medical students and variation exists amongst individual Australian medical faculties, between states as well as individual universities from the same state. Furthermore, there is very little teaching here in Australia in relation to emerging genomic technologies within oncology, and in particular, the ever-increasing role of personalised and preventative medicine in cancer care today. Ultimately, there is a clear need for an integrated, overarching national oncology curriculum, embracing a patient-centred approach; national evaluation and assessment; supplementary courses; utilisation of self-directed learning and reflective practice activities; and greater emphasis on emerging technologies. With more research focus on this area, in future there may be a larger evidence-base targeted at providing improvements in Australian Oncology education, assisting graduates in gaining adequate understanding and appreciation of cancer-related scenarios and cancer care. More effective teaching and learning facilitation, with better overall Australian training outcomes, will lead to advancement in cancer diagnosis, treatment, and management as well as ensuring more insightful and valuable patient interactions in the future.
Introduction
A multitude of changes are revolutionising the study and practice of oncology worldwide. The ways in which oncology and cancer care are incorporated into medical school curricula in Australia is thus of particular interest. Despire the undeniable importance of cancer education, there is currently no consensus amongst Australian medical schools as to what should be taught in regards to oncology practice, nor have the best ways of teaching and learning about cancer and cancer care been fully elucidated in the literature or in the clinical realm [1-4].
In Australia, there is considerable variation in undergraduate and postgraduate teaching of oncology amongst individual medical faculties [8,9] and a lack of important cancer knowledge amongst graduating medical students, between states and between individual universities from the same state [8,9,10]. This inconsistency is compounded by the nature of oncology as a multidisciplinary specialty, with overlap in numerous fields including pathology, surgery, histology, radiology, anatomy, genetics, communication skills, and palliative care [1].
Further, there is very little teaching here in Australia in relation to emerging technologies within oncology and in particular, the ever-increasing role of personalised and preventative medicine in cancer care today. Educators are now presented with the inevitable task of addressing all foundational educational needs in our generation of medical graduates. They must also ensure to incorporate pertinent aspects of such a rapidly progressive field of medicine as it relates, for example, to genetic testing and counselling, the rise of personalised or ‘precision’ medicine, and ongoing development in cancer immunotherapies [11-14].
Variation in oncology education in Australia is compounded by the lack of literature on this subject, which is predominantly qualitative in nature and overall, more difficult to evaluate [30]. Whilst cancer is the number one cause of death in Australia, oncology itself is still not a subscribed part of the medical curriculum, nor is an oncology rotation compulsory in Australian medical schools. There is an ongoing lack of literature regarding oncology-specific teaching and learning methods, as well as a lack of evidence in the effective implementation of compulsory curricula or rotations to engage with foundational and emerging aspects of oncology or palliative care.
The importance of this issue resonates with students, recent graduates, and educators as all medical students will at some point in their career play a role in the management of a cancer patient [5], whether as a resident on an oncology rotation, as a general practitioner at the stage of diagnosis, during long-term follow-up of a cancer survivor [6], as a fully-qualified oncologist, or as a clinical geneticist. Furthermore, with our ageing Australian population, there will be greater numbers of individuals diagnosed with and treated for cancer than ever before as well as an increased number of survivors, making cancer a chronic illness to be managed by a multidisciplinary team [7].
How did we get here?
In 1993, the General Medical Council published a detailed review of medical education [15], which led to a major overhaul of medical school oncology training in the United Kingdom, and worldwide [1,16]. A survey of European universities showed that 95% indicated the need for increased cancer education and there was an overwhelming interest in a common European oncology curriculum [17].
In 1999, and again in 2007, the Ideal Oncology Curriculum (IOC) for Medical Students was released here in Australia [18], produced by the Oncology Education Committee of the Cancer Council Australia and endorsed by the Union for International Cancer Control (UICC). It provides an unparalleled example of the evidence-based recommendations required for medical school cancer education, including prescribed clinical experiences and knowledge attainment, which necessitate a patient-centred approach to training methods. In each section, there is detail of prerequisite knowledge, as well as a list of representative questions that illustrate the ‘required depth of knowledge’ for graduating medical students, with attached example answers and multiple-choice question-answer options.
Focus is on the patient rather than the discipline, with topics ranging from public health and cancer biology, to patient management, diagnosis, communication skills, and clinical experiences [18]. More recently, it has been supplemented by a detailed e-Book entitled “Clinical Oncology for Medical Students”, which may be utilised alongside the recommended experiential learning, and acquisition of technical oncology skills, for a more robust understanding of the prescribed IOC material [19].
Moreover, the World Health Organisation and UICC recommend that cancer education be incorporated into oncology modules within an undergraduate curriculum and that medical students spend a minimum of two weeks in oncology training [4,5]. However, despite the superlative example given by the IOC, there has been minimal uptake in Australia, which may be linked to the current lack of a national curriculum, the dearth of literature on effective educational strategies, or the historical absence of oncology content in Australian medical school curricula. This lack of implementation and an inadequate evidence-base makes the feasibility and effectiveness of oncology rotations or uptake of the IOC guidelines incredibly difficult to ascertain, let alone, achieve.
Oncology teaching and learning methods
Internationally, there has been a push for an overarching pre-clinical oncology curriculum for medical students incorporating medical knowledge, psychosocial aspects, communication skills training, and utilisation of a variety of teaching methods such as interviews, discussion, reflection, and lectures [1,2,7,20].
There is increased emphasis on a patient-centred approach to teaching [11,13] and learning in oncology education [22,23]. This should extend from the use of standardised patients teaching examination skills to medical students, to the involvement of cancer patients in communication skills teaching and portfolio learning [1,24].
Self-directed learning (SDL) is the educational strategy considered most likely to produce medical graduates who are prepared for lifelong learning and who are able to meet the needs of their patients [26,30]. SDL activities include problem-based learning (PBL), discovery learning, task-based learning, experiential and reflective learning, portfolio-based learning, small group or project-based learning, and peer evaluation with learning contracts [26]. Results from numerous studies have indicated a trend towards improved student performance from SDL assessment, as with the follow-up of a cancer patient over an extended period of time [1,21,23-25]. The use of portfolio assessment and learning journals is also championed as a tool of successful oncology training and for lifelong education [25]. An array of methods may thus be employed in undergraduate oncology training whilst utilising the SDL approach [26-27].
The PBL approach, more specifically, as one of the major aspects of SDL, facilitates a deeper learning style [28] and involves an active search for understanding based on a given scenario. This technique is linked to better clinical problem-solving skills in medical students with higher levels of motivation and stimulation found [27] and superior outcomes in students tested [9,29].
Regarding format, some have argued that an independent block style is more effective in presenting an oncology curriculum [20]. This is as opposed to an integrated model of teaching into other system modules and would be relevant within an Australian-based system. In block format, the curriculum may be presented through oncology-specific technology-based lectures, team-based communication, and clinical skill exercises supplemented by lectures paired with relevant clinically-based scenarios and other activities posted online to be worked through independently [20].
Computer-aided learning [1,21,22,30] may itself have a role to play as supplementation to oncology study though technology-based approaches are not necessarily superior to other learning techniques [1]. Here in Australia, a number of medical schools are already utilising the e-Learning Undergraduate Modules for Australian Medical Schools, accessible via The e-Learning Portal, which is provided by The Australasian College of Dermatologists [31]. This is highly applicable on a national level when considering skin cancer rates in Australia [32]. Overseas, an ‘eDerm’ online curriculum [33] provided to 252 medical students in the United States significantly improved the diagnosis and management of pigmented skin lesions by medical students [33].
In regards to communication skills, suboptimal communication can lead to adverse psychological effects in patients. It can compromise a physician’s ability to treat patients, as well as impacting patient satisfaction, medication compliance and overall clinical outcomes [34]. The use of group presentations, small-group communication skills practice [35], and reflective self-awareness exercises have been shown to improve communication skills. This is particularly true with the use of patient-actors in simulated clinical situations as opposed to role-play alone. There is overwhelming proof that communication skills can be taught and should be delivered through experiential learning methods, which are ultimately more effective than instructional modes to address communication skills development in oncology [36].
Moreover, a primary skill that any medical student can bring to an oncology experience, or rotation is their presence and their time. Medical student training in this burgeoning field [11] must facilitate the development of essential communicative abilities: to be able to listen to a cancer patient’s story during their clinical journey, to be able to connect with this experience, and communicate effectively in response to this scenario [18,34-36].
Lessons from abroad
At the University of Wales’ College of Medicine, medical students followed a patient along their cancer journey over a six-month period and were assessed during patient interactions and through a final portfolio. Overall, students found the project rewarding and reported gaining unparalleled insight into the cancer experience [22].
A three-day intensive oncology course has been piloted in Israel, with students feeling more comfortable with cancer-related issues, less afraid of dealing with death, and better able to cope with uncomfortable cancer-related emotional situations as a result [7]. Psychosocial and ethical aspects were presented through student-led presentations and discussions, a psycho-oncology session led by a psychologist, and two presentations by cancer patients describing their personal experiences and offering advice on aspects such as the doctor-patient relationship [7].
In Poland, attempts have been made to improve cancer education through the National Program for Combating Neoplastic Diseases [16]. This was done with a course incorporating computer-learning modules, online tests, portfolio learning, summer school, modules taught by cancer patients, and attachments in oncology and palliative care. Observations highlighted that the introduction of these courses better prepares students for delivering cancer care [16].
Finally, in a novel Brazilian experience, students staffed an oncology clinic, with 77% of students involved in this approach over a ten-year period rating it as the best activity of their course. Findings suggested that attendance at an oncology outpatient clinic can contribute significantly to the cancer education of medical students [24].
Future directions for Australian oncology education
There is a clear need for the following in cancer education:
An integrated, overarching national curriculum, with a patient-centred approach
National evaluation and assessment
Summer schools and supplementary courses
Embracing SDL & PBL, with reflective practice activities
Greater emphasis on emerging technologies
An oncology curriculum, with a patient-centred approach
A relevant, integrated oncology curriculum as detailed by the IOC [15,18] should be embraced by all Australian medical schools, with the aim of bringing together requirements regarding essential knowledge, skills, and attitudes about cancer and cancer-related care [2,8,9,10,17]. It should be well-rounded and ideally supported by a coordinating body, with an academic basis of professorships [2].
As detailed by the IOC [18], there is a need for increased emphasis on clinical interaction and greater time spent with patients [1,2,5,21,37]. As suggested [18], medical students need at least five cancer clinical experiences before graduating:
Talking with and examining people affected by all stages of cancer;
Talking with and examining people affected by all common cancers;
Observing all components of multidisciplinary cancer care;
Seeing shared decision-making between cancer patients and their doctors; and
Talking with and examining dying people [2,15,18].
Assessment
As shown in Australian medical schools, assessment drives performance [2]. Thus, having decided upon a particular patient-centred approach, carrying out formal evaluation of student learning and course content is vital for enhancing training outcomes [18,38], and should inform the prescribed curriculum [2]. In future, this might include the introduction of national assessment, such as a national exit examination [40], with oncology-related scenarios aimed at testing core knowledge levels and ensuring standardisation is maintained across the country [9,39,40].
Supplementary courses
Regarding adjuncts to a proposed national curriculum and module [20] of oncology teaching, summer schools and extra courses [7,16] may be of great use here in Australia [1]. The Vienna Summer School, for example, receives high levels of praise and acceptance rates from European medical students. These students note that these supplementary courses provide them with a greater understanding of oncology and an appreciation of its’ multidisciplinary character [15]. Summer schools may offer educational activities that fill the gaps of an otherwise disjointed oncology training program, as shown by the example of oncology summer schools in Europe [4].
Self-directed learning, problem-based learning and reflective practice
Learning in medical school is rarely fully autonomous, with students valuing pedagogic support and often relying on teachers as coordinators and facilitators of their learning environment [41]. Students should be encouraged to recognise the importance of evidence-based medicine, how to critically appraise literature, and the need to constantly update one’s knowledge based on high-quality evidence and guidelines [18]. Furthermore, team-based learning through small scenario or discussion groups has a role to play in the application of basic science knowledge to real-world oncology-related scenarios [35]. This could lead to greater engagement with lecture content and its’ application in daily medical practice.
There is increasing necessity for our medical curriculum to foster the development of sound communication skills. Furthermore, providing students at every level of their education with an opportunity for reflective practice, as individuals and in smaller groups, is also a must. This may serve as an important tool in supporting students who emotionally encounter negative experiences as a result of difficult or uncomfortable clinical encounters. Mentoring, as an extension of this pathway, may be of use in allowing reflection following hospital experiences. It may be of use for medical students to attach themselves to ‘mentor’ clinicians on rotation, staff whom they perceive to be effective teachers for coaching purposes, development of reflective practice, and consolidation of learning [42].
Moreover, students learn more effectively by being actively involved in a PBL strategy, as it facilitates epistemic curiosity through activation and elaboration of prior knowledge [22]. Reflection on experience, followed by evaluation, analysis, and appropriate action, may facilitate further learning and appreciation of curriculum content in the Australian context [1,4,18,21,22,23,25]. Portfolio learning [1,22,23] should thus be employed in a set teaching program [16,23], with reflective exercise and a compulsory portfolio-based experience, or assessment. This would to facilitate reflection and exploration of the patient experience along their cancer trajectory.
Emphasis on emerging technologies
Dramatic advances in genomic technology stand to revolutionise clinical cancer care [13,14]. Personalised (or ‘precision’) medicine is a banner term, describing the use of molecular tools to individualise healthcare through genetic testing, whole genome sequencing, exome, or transcriptome sequencing [13]. While there has been ample research in the area of genetic testing and its’ implications for our future, very little is known about how best to encourage development in understanding of such technologies at the level of medical students or recent graduates.
In the realm of breast cancer in Australia, for example, an individualised cancer care approach is evidenced in the case of genetic testing for BRCA1/2 mutations, which reflect a specific predisposition toward breast and ovarian cancer [43]. About 5% of cases of breast cancer and 10% of ovarian cancer cases, are due to such inherited predisposition [44,45]. With progress towards a more personalised, family-centred model of oncological care in Australia, knowledge of ones’ genetic and genomic information plays a crucial role, from screening and prevention, to individualised surgical treatment, and utilisation of targeted therapies based on a tumours’ molecular signature [46].
In order to fully realise the effective application of personalised medicine into routine Australian cancer care, students and clinicians need a more comprehensive understanding of emerging technologies. In addition, an appreciation of the experiences, and attitudes of cancer patients, and their families is required. Evidence suggests that the majority of cancer patients are willing to undergo genetic and genomic testing during, or following, cancer treatment [11]. More work is needed in this area to provide graduates with a more refined appreciation of how best to communicate genomic concepts to a broad range of patients [11]. Medical graduates must have greater awareness of foundational genetics-based and personalised medicine pathways. This will allow them to alleviate patient misconceptions and ultimately, to empower patients to make more informed cancer care decisions [12-14]. Without this, there may be failure to adequately deliver genetically-guided cancer care, treatment, and management in the future. The issue our educators will now face is how to best integrate this information into a feasible medical student curriculum.
Conclusion
More effective teaching and learning strategies in oncology should be aimed at producing Australian medical graduates with adequate and relevant cancer-related knowledge, skills, and attitudes that best meet the needs of their society [2]. The IOC [18] does an exceptional job of demonstrating the requirements and expected knowledge to be attained through a prescribed oncology curriculum here in Australia.
Australian medical students need a well-rounded understanding of oncology concepts and appropriate examination and communication techniques to facilitate aspects of cancer diagnosis, referral, and management in future clinical practice [20]. There must be focus given to developing an awareness of emerging technologies in the realm of cancer care with emphasis on basic concepts related specifically to genetic testing, genetic counselling, and personalised medicine.
The foundational experiences provided by medical school training serve to shape one’s entire career as a doctor. Those students more engaged in their learning through SDL, PBL and reflective practice strategies [26,27], and who have a greater understanding of key concepts are more likely to achieve superior assessment outcomes [2]. They are also more likely to be involved in successful clinical interactions overall [1].
With greater research focus on this area in future, there may be a larger evidence-base targeted at providing overarching improvements in Australian oncology education. This will assist graduates in gaining an adequate understanding and an appreciation of cancer-related scenarios and cancer care. More effective teaching and learning facilitation with better overall Australian training outcomes will ultimately lead to advancement in cancer diagnosis, treatment, and management outcomes as well as ensuring more insightful and valuable patient interactions in our futures [5,12].
Conflicts of interest
None declared.
References
Gaffan J, Dacre J, Jones A. Educating undergraduate medical students about oncology: a literature review. Journal of clinical oncology. 2006;24(12):1932-9.
Barton MB, Bell P, Sabesan S, Koczwara B. What should doctors know about cancer? Undegraduate medical education from a societal perspective. The Lancet Oncology. 2006;7(7):596-601.
Fromm-Haidenberger S, Pohl G, Widder J, Kren G, Fitzal F, Bartsch R, et al. Vienna international summer school on experimental and clinical oncology for medical students: an Austrian cancer education project. Journal of Cancer Education. 2010;25(1):51-4.
Pavlidis N, Vermorken JB, Stahel R, Bernier J, Cervantes A, Audisio R, et al. Oncology for medical students:: A European School of Oncology contribution to undergraduate cancer education. Cancer Treatment Reviews. 2007;33(5):419-26.
Payne S, Burke D, Mansi J, Jones A, Norton A, Joffe J, et al. Discordance between cancer prevalence and training: a need for an increase in oncology education. Clinical Medicine. 2013;13(1):50-6.
Practitioners RACoG. The RACGP Curriculum for Australian General Practice: RACGP 2016 Curriculum. Melbourne: The Royal Australasian College of General Practitioners. 2016.
Granek L, Mizrakli Y, Ariad S, Jotkowitz A, Geffen DB. Impact of a 3-Day Introductory Oncology Course on First-Year International Medical Students. Journal of Cancer Education. 2016:1-7.
Smith WT, Tattersall MHN, Irwig LM, Langlands AO. Undergraduate education about cancer. European Journal of Cancer and Clinical Oncology. 1991;27(11):1448-53.
McGrath BP, Graham IS, Crotty BJ, Jolly BC. Lack of integration of medical education in Australia: the need for change. Medical journal of Australia. 2006;184(7):346.
Tattersall MHN, Langlands AO, Smith W, Irwig L. Undergraduate education about cancer. A survey of clinical oncologists and clinicians responsible for cancer teaching in Australian medical schools. European Journal of Cancer. 1993;29(11):1639-42.
Gray SW, Hicks-Courant K, Lathan CS, Garraway L, Park ER, Weeks (2012). Attitudes of patients with cancer about personalized medicine and somatic genetic testing. Journal of Oncology Practice; 8(6): 329-35.
McGowan ML, Settersten RA Jr, Juengst ET, Fishman JR. (2014). Integrating genomics into clinical oncology: ethical and social challenges from proponents of personalized medicine. Urologic Oncology; 32(2): 187-92.
Tian Q, Price ND, Hood L. (2012). Systems cancer medicine: towards realization of predictive, preventive, personalized and participatory (P4) medicine. Journal of Internal Medicine; 271(2): 111-21.
Ward RL. (2014). A decade of promises in personalised cancer medicine: is the honeymoon over? The Medical Journal of Australia; 200(3): 132-3.
General Medical Council. Education C. Tomorrow’s doctors: recommendations on undergraduate medical education: General Medical Council London; 1993.
Matkowski R, Szelachowska J, Szewczyk K, Staszek-Szewczyk U, Kornafel J. Improvements in undergraduate oncology education introduced at Polish Medical Universities between 2004 and 2010 under Poland’s “National Program for Combating Neoplastic Diseases”. Journal of Cancer Education. 2014;29(3):428-33.
Robert KH, Einhorn J, Kornhuber B, Peckham M, Zittoun R. European undergraduate education in oncology: a report of the eortc Education Branch. Acta Oncologica. 1988;27(4):423-5.
Oncology Education Committee. Ideal oncology curriculum for medical schools. The Cancer Council Australia. 2007.
DeNunzio NJ, Joseph L, Handal R, Agarwal A, Ahuja D, Hirsch AE. Devising the Optimal Preclinical Oncology Curriculum for Undergraduate Medical Students in the United States. Journal of Cancer Education. 2013;28(2):228-36.
Matkowski R, Szelachowska J, Szewczyk K, Staszek-Szewczyk U, Kornafel J. Improvements in undergraduate oncology education introduced at Polish Medical Universities between 2004 and 2010 under Poland’s “National Program for Combating Neoplastic Diseases”. Journal of Cancer Education. 2014;29(3):428-33.
Maughan TS, Finlay IG, Webster DJ. Portfolio learning with cancer patients: an integrated module in undergraduate medical education. Clinical Oncology. 2001;13(1):44-9.
Finlay IG, Maughan TS, Webster DJT. A randomized controlled study of portfolio learning in undergraduate cancer education. MEDICAL EDUCATION-OXFORD-. 1998;32:172-6.
Abrão MN, Bensi CG, Gonçalves MS, Narahara JL, Otsuka FC, Ranzatti RP, et al. A medical student-staffed outpatient oncology clinic: a 10-year Brazilian experience. Journal of Cancer Education. 2008;23(1):63-4.
Orr B. Learning in oncology: lessons from the 20th century, learner-centred education for the 21st century: part II. Clinical oncology. 2004;16(6):435-8.
Spencer JA, Jordan RK. Learner centred approaches in medical education. British Medical Journal. 1999;318(7193):1280.
Barrows HS. Problem-based learning in medicine and beyond: A brief overview. New Directions for Teaching and Learning. 1996;1996(68):3-12.
Newble DI, Entwistle NJ. Learning styles and approaches: implications for medical education. Medical Education. 1986;20(3):162-75.
Newble DI, Clarke RM. The approaches to learning of students in a traditional and in an innovative problem-based medical school. Medical Education. 1986;20(4):267-73.
Coles CE, Spooner D. Lifelong learning in clinical oncology editorial series: introduction and overview. Clinical Oncology. 2011;23(5):309-11.
The Australasian College of Dermatologists. 2016. ACD e-Learning Portal. Australia: The Australasian College of Dermatologists.
Australian Institute of Health and Welfare. AIoHaWC. Cancer in Australia: an overview, 2014. . Cancer series no 78 Cat no CAN 75 2014.
Dolev JC, O’Sullivan P, Berger T. The eDerm online curriculum: a randomized study of effective skin cancer teaching to medical students. Journal of the American Academy of Dermatology. 2011;65(6):e165-e71.
Back AL, Arnold RM, Tulsky JA, Baile WF, Fryer-Edwards KA. Teaching Communication Skills to Medical Oncology Fellows. Journal of Clinical Oncology. 2003;21(12):2433-6.
Haidet P, O’Malley KJ, Richards B. An Initial Experience with “Team Learning” in Medical Education. Academic Medicine. 2002;77(1):40-4.
Aspegren K. BEME Guide No. 2: Teaching and learning communication skills in medicine-a review with quality grading of articles. Medical teacher. 1999;21(6):563-70.
Cave J, Woolf K, Dacre J, Potts HWW, Jones A. Medical student teaching in the UK: how well are newly qualified doctors prepared for their role caring for patients with cancer in hospital? British journal of cancer. 2007;97(4):472-8.
Dennis KEB, Duncan G. Radiation oncology in undergraduate medical education: a literature review. International Journal of Radiation Oncology* Biology* Physics. 2010;76(3):649-55.
Koczwara B, Tattersall MHN, Barton MB, Coventry BJ. Achieving equal standards in medical student education: is a national exit examination the answer? Medical journal of Australia. 2005;182(5):228.
Lawson-Smith C. Achieving equal standards in medical student education: is a national exit examination the answer? The Medical journal of Australia. 2005;183(3):167.
Dornan T, Hadfield J, Brown M, Boshuizen H, Scherpbier A. How can medical students learn in a self‐directed way in the clinical environment? Design‐based research. Medical education. 2005;39(4):356-64.
Norman GR, Vleuten C, Newble D. (2002). International handbook of research in medical education. Boston: Kluwer Academic.
Komatsu H, Yagasaki K. Are we ready for personalized cancer risk management? The view from breast-care providers. International Journal of Nursing Practice 2014; 20(1): 39-45.
Di Prospero LS, Seminsky M, Honeyford J, et al. Psychosocial issues following a positive result of genetic testing for BRCA1 and BRCA2 mutations: Findings from a focus group and a needs-assessment survey. Cmaj 2001; 164(7): 1005-9.
Doherty GMW, L.W. Current Diagnosis & Treatment: Surgery (14th ed.). New York: McGraw-Hill Medical; 2015.
Fashoyin-Aje L, Sanghavi K, Bjornard K, Bodurtha J. Integrating genetic and genomic information into effective cancer care in diverse populations. Annals of Oncology 2013; 24 Suppl 7: vii48-54.
Alzheimer’s disease is a commonly encountered pa ent case by medical students. However, many students struggle to see the person beyond the disease. This essay o ers a di erent perspec ve into Alzheimer’s disease, a deeper understanding that is crucial towards fostering more empathe c, a en ve and compassionate pa ent interac ons.
Since the start of my medical studies, I have found the disease process of Alzheimer’s disease an emotional and physiological enigma. However, it is the case of Clarice that profoundly impacted a deeper insight into the complexity of a life lived with Alzheimer’s disease.
Clarice has been living with Alzheimer’s disease since the death of her husband eleven years ago. Her family helplessly witness as she gradually loses any semblance of order and familiarity in her life. At first, she disguised her confusion through a veil of phrases, covering up her forgetfulness with laughter “Of course I knew that, I was only joking.” Alzheimer’s disease drowned Clarice within waves of confusion, muddling up her thoughts and blending the faces she was surrounded by all of her life with faces of strangers as she tried to tread water in the relentless current. She always wore a smile and came accompanied with jokes and quirky musings. She became known by eccentric catch phrases “How do you spell nachas (happiness)?” that she asked of her grandchildren. To which they answered melodiously “C L A R I C E”. At every family gathering, she tapped her glass with a fork and announced, “with tears in my eyes, I just want to say how special it is to be here, no itching or bitching, just all together, as a family.” As she left, she gathered everyone together and departed with famous final words “Go well, go shell, but don’t go to hell”.
“Go well, go shell, but –“,
“Don’t ring the bell!”
“Don’t say farewell!” her family tried to interject.
“No.” she confirmed with a cheeky grin, “Don’t go to hell!”
At Friday night meals, Clarice’s thirteen grandchildren said the Jewish blessing over food in chronological order from eldest to youngest. With much humour, Clarice would exclaim “Our Father, the holy spirit…” and proceed to tap out the cross on her body, reminding them of her rich childhood. Having attended a Catholic boarding school as a young Jewish girl, the daily prayers and hymns have stayed with her into old age. Her family loved her Zulu exclamations “saqua bona wena”, to which they replied in their own made up language, matching the sounds of her youth.
As her cognition declined, her honesty and humour sharpened and the kindness, love, and compassion that overflowed from her heart amplified. At times, her honesty was brutal, revealing hidden layers about the people surrounding her. No longer aware of social cues or the importance of privacy, she pointed out the sad man sitting by himself, or the distressed woman lost in thought. While sometimes uncomfortable, such honesty only exposed her caring and sensitive nature. She was apt at identifying someone’s hidden sadness, unbeknownst to anyone else, and quick to enquire why, offering her ear and heart.
If her family had visitors at their weekly Shabbat meals who showed signs of fragility, Clarice was the first to get up and help. “Can I help you up from the table?” “You stay put and I’ll get your food for you, what would you like?” The irony of such moments was heartrending, her ability to help those who were physically unwell when she wasn’t able, nor was anyone else, to help the illness that overwhelmed her mind.
As time gradually undid the threads that held together the clarity of Clarice’s mind, her sentences slipped into nonsensical musings. Moments of her childhood featured more frequently as she lost track of time. She referred to herself as a little girl, telling her adult children that she had to go home lest her parents worry where she was.
Yet, there were moments of pure happiness that peaked out occasionally. Her genuine awe as she watched the sunsets that showered her balcony and the raw happiness and surprise she had when her granddaughters kissed her on the cheek for a ‘selfie’, were moments of bliss. Her family learnt what made her happy and was able to tap into such experiences to change solemn moments into happier ones. The more they became desensitised to the tragedy of her illogical talk and the more they learnt how to laugh with her rather than cry, the more they were able to find joy and beauty in her quirky musings and disjointed sentences. The more they distanced themselves from her disease, the more they appreciated her presence, her warmth, and her unconditional love.
Clarice is not and never has been my patient. She is my grandmother, my Bobba. At the same time that I was dealing with the sudden deterioration of my Bobba’s cognition, I started my geriatrics placement at the hospital. The internal struggle that I felt as I grappled with my Bobba’s decline gave me a new perspective of the patients I met during that term.
Patient labels transitioned from ‘the demented old lady with delirium secondary to constipation’ to ‘the retired teacher and grandmother of seven suffering with …’. I found myself with a newfound depth of empathy and patient centered care. This gave me a greater understanding of the underlying disease processes of the patients as my passion for their wellbeing led me to deeper investigations of their conditions. The lessons I learnt from communicating with my Bobba, especially in her moments of stress and confusion, enabled me to connect to the geriatric patients with greater patience, tolerance, and appreciation. I found that I was able to implement the ‘tricks’ I learnt from soothing my Bobba to soothing distressed, agitated, and scared patients. The timing of my geriatrics placement was no coincidence but a treasured journey that transformed the blanket of grief, loss, and regret that plagued my mind, with acceptance, gratitude, and understanding. It was emotionally draining to be confronted with the exact challenges that I tried to distance myself from in my personal life every day at placement. Nonetheless, witnessing so many people in the same circumstance as my Bobba and my family also brought solace and comfort.
One moment I will never forget was walking into a very disorientated woman’s room; she was 63 years old and had early onset Alzheimer’s disease. She lay in bed with her 40-year-old daughter, who cuddled her while stroking her hair and placating her with kind words “Don’t worry mum, I’m here, everything’s going to be alright”. I left hospital that day and went straight to my Bobba’s home. Although I sensed that she didn’t know exactly who I was that day, I felt her love for me and as we sat together cuddled up on the couch, I found pleasure in the complex simplicity of love and togetherness that persists, and perhaps even strengthens, in the face of suffering and adversity.
Just like the 40-year-old daughter, I remember my own mother placating my Bobba by likening her confusion to a car ride, telling her that she can simply shut off, relax, and enjoy the ride, knowing with confidence that she was being looked after. That although she was in the passenger seat, she could trust in the fact that the driver had planned the journey meticulously ahead with love and care. When my mother suffered herself, overwhelmed by hopelessness and pain, I remember my aunty, my mother’s younger sister, telling her that it was better to laugh, to simply shut off, relax, and enjoy the ride herself. As my aunty so aptly put it, “we have to laugh, for if we don’t laugh, then we’ll just cry.”
We chose to ignore the ugliness of the disease and to find joy in the benevolent absurdity of my Bobba’s behaviour. We laughed in the lift of crowded people when my Bobba interrupted the silence singing ‘Ba Ba Black Sheep’. We laughed when my Bobba plaited my friends’ hair together as they sat on the couch. We laughed when my Bobba walked up to the stranger engrossed in her book to sit down beside her and engage in conversation as if they were lifelong friends. We laughed so much with my Bobba until we laughed so much that we cried. And I thought of all those times we ran around as small children, my Bobba warning us “too much laughter ends in crying”. Yet, now we reversed this, we turned all our crying into laughter. And we were so much happier.
Alzheimer’s disease teaches us to savour every minute spent with those we love. It sensitises us to those extraordinary moments of pure joy. It clears out the complexity of the recent past and future to make way for the serenity of the present. It peels away the shell of the mind only to reveal the perfection of the soul – what a beautiful force to be around.
Conflicts of Interest
None declared.
This article was first published in the Australian Journal of Dementia Care (www.journalofdementiacare.com) Vol 5 No 6 December/January 2016-2017. Reprinted here with the permission of Hawker Publications Australia Pty Ltd.
Background: Acquired brain injury (ABI) in childhood can have serious physical, cognitive, and social consequences, although its specific impact on schooling attendance and provision of aid for children is often uncertain. We described educational and neuropsychological outcomes for a population of children with moderate to severe ABI.
Methods: A retrospective cohort study of children with moderate to severe ABI attending a paediatric brain injury service at The Children’s Hospital at Westmead between January 2003 and December 2007 was performed. The children were aged 8-16 at time of injury and information on school attendance, provision of aide, and neuropsychological test results were collected at 6, 18, and 30 months post-injury. Children with previous moderate to severe ABI, neurological disorders or learning difficulties were excluded.
Results: 104 children were included (mean age 12.4, 62.5% male). 48 had severe ABI (Glasgow Coma Scale ≤ 8 or Post Traumatic Amnesia ≥ 7 days). The proportion having returned to full time schooling improved from 56% to 89.7% between the 6 and 30-month follow-up. A majority of children had an impairment recorded on neuropsychological testing. Regression analysis found that severity of injury and language deficit were predictors of attendance in the first six months post-injury. During the 30-month follow-up, 18% of children attended special classes or received a classroom aide.
Conclusion: Time is important in recovery from ABI in children. Neuropsychological deficits influence delivery of classroom aides or modified curricula. Children with severe injury are more likely to have poorer cognitive and educational outcomes.
What is already known about this topic
Acquired brain injury can lead to serious physical, mental, and social problems for school-aged children
These deficits can often extend years after the initial injury
Severity of injury is correlated with poorer outcomes
What this paper adds
An Australian perspective of educational outcomes for children with moderate to severe brain injury
Information on deficits experienced by children over two-and-a-half years of follow-up
A better understanding of the importance of time, neuropsychological deficits, and physical injuries in transition back to school
Introduction
Acquired brain injury (ABI) includes a range of disabilities affecting the brain after birth including traumatic brain injury and haemorrhage. Children with moderate to severe ABI often experience long-term physical, cognitive, or behavioural impairments [1,2]. During discharge planning for these children, families often want to know what to expect from the future. In particular, they worry about the transition from hospital to the home and school environment [3]. Schooling is an important forum for childhood learning, as well as emotional and social development [4]. As such, parents often worry about how and when their children may return to school [5]. These concerns are important to address but are difficult to answer due to the great heterogeneity of outcomes following ABI.
Research has indicated that transition of children with ABI back into school is a challenging time for families. After brain injury, students may need to change their educational and vocational goals to accommodate changes in their abilities [6]. Interviews with children returning to school after ABI raise many issues, including social isolation, missed schoolwork, difficulties adjusting to physical and cognitive changes, and the support provided by schools [7]. Children find it more challenging to participate in school activities than at home and this may be due to the familiarity and greater support provided by the home environment [8].
It has been clearly established by prospective longitudinal studies that severity of injury is associated with poorer physical or cognitive outcomes [1,9-11]. Younger children are also more vulnerable to ongoing consequences of brain injury due to their larger head-to-body ratio, ongoing brain tissue myelination, and their thinner cranial bones [12]. Other factors such as type of injury, socioeconomic status, and provision of family support are also known to affect outcomes following childhood ABI [1,5,7]. Time plays a particularly important role in recovery from ABI however it is useful to note that some deficits may also become more apparent over time.
Neuropsychological testing may also be an early predictor of educational performance and special education requirements: in a study by Kinsella et al., severity of injury and verbal memory and fluency at three months post-injury was a predictor for requirement of special education at 24 months post-injury, Similar findings of the importance of verbal memory influencing educational performance at two years post-injury were made by Catroppa and Anderson as well as Miller and Donders [13,14]. Arnett also found that measures of executive functioning and verbal memory predicted educational competency but did not find these measures predictive of provision of special education [15]. Many studies regarding educational and schooling outcomes for children with ABI do not look specifically at school attendance. Studies of educational outcomes are also limited by small patient numbers and limited follow-up [16].
This study aims to use retrospective data to provide a better understanding of specific neuropsychological and schooling outcomes for children with moderate to severe ABI over a two-and-a-half-year period of follow-up. In particular, the study looks at providing a picture of time for return to schooling and the likelihood of requirement for an aide in the classroom or special education. It also seeks to explore whether neuropsychological factors such as attention, memory, information processing, and executive function, and whether co-morbidities such as fatigue and motor capacity may influence return to school and provision of an aide. This information may enable parents of children with ABI to have a better understanding of what to expect and could improve school engagement in the rehabilitation process [7].
Methods
Participants
Eligible cases were identified from the 2003-2007 database of a paediatric brain injury service at The Children’s Hospital at Westmead, New South Wales, Australia.
Inclusion criteria were age at injury of 8-16 years, moderate or severe ABI, and admission to hospital for ABI. Moderate ABI was defined as Glasgow Coma Scale (GCS) ≤ 12 or Post Traumatic Amnesia (PTA) ≥ 1 day. Severe ABI was defined as GCS ≤ 8 or PTA ≥ 7 days [17]. There were eight cases which were judged as representing moderate or severe ABI but there was unclear GCS and PTA data. These cases were included in order to more accurately represent the patient population and were classified as “undefined” in severity.
Exclusion criteria were previous moderate or severe ABI, previously documented behavioural or developmental difficulties, or previously documented special education support.
Medical records were searched and data extracted from neuropsychological and brain injury clinic reports, discharge summaries, and other hospital records. Data were collected for 0-6, 6-18, and 18-30 months post-injury. Data on educational outcomes of school attendance, provision of classroom aide, and whether children changed school were collected. Data on neuropsychological outcomes was taken from reports written by clinical neuropsychologists at the service. Patient demographics were taken from medical notes. Information on co-morbidities was collected primarily from brain injury clinic reports.
Measures
The neuropsychological testing variables measured were attention, memory, information processing, and executive functioning. Neuropsychological profile was considered intact when reported as “low average” or above. Where terms such as “difficulty”, “reduced”, “borderline”, or “impaired” were used as descriptors in reports they were coded as a deficit. In cases where children had no deficit on initial neuropsychological testing and were subsequently discharged without further testing, it was assumed that they would not develop deficit later on.
This research also collected data on variables concerning other sequelae of ABI including mood/behavior, fatigue, gross and fine motor deficit, receptive and expressive language deficit, visual impairment, and hearing impairment. These deficits were determined by whether they were mentioned as ongoing issues in clinical letters and other medical notes during the set follow-up periods.
Statistical analysis
Quantitative analysis was undertaken using STATA 11 SE. Where possible, variables were coded dichotomously for analysis using Fisher’s Exact Test to look for a relationship with attendance at school or provision of aide. Ordered logistical regression examined which variables (severity, neurological findings, or co-morbidities) were predictive of school attendance.
Ethics approval
Ethics approval was obtained from the Services Improvement Unit at The Children’s Hospital at Westmead, NSW, Australia, approval number: QIE-2011-02-09.
Results
Participant demographics (Table 1)
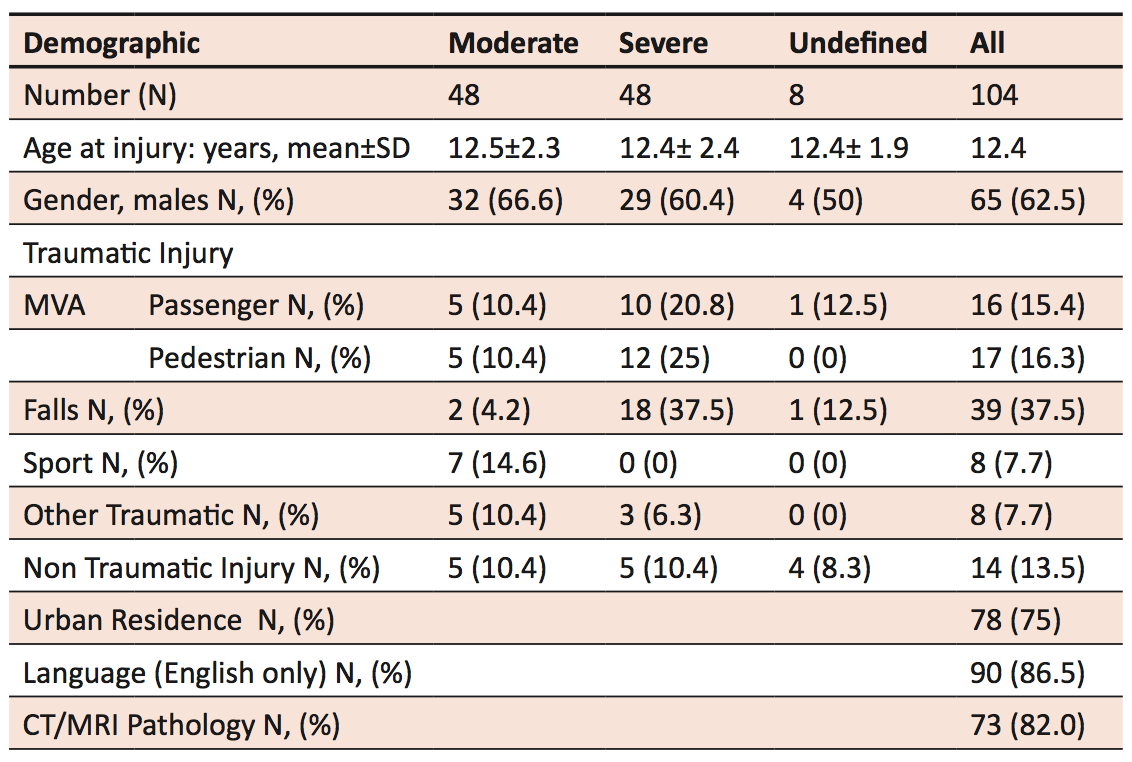
Of the 158 identified cases, 104 cases met the inclusion criteria. Age at time of injury was between 8-16 years, with the mean age at time of injury being 12.4 years. There were 48 children with severe injury, 48 with moderate injury and 1Table 1.)vehicle accidents. CT/8 with non-traumatic injury, mostly haemorrhage from rupture of arteriovenous malformations. 62.5% were male and three quarters came from urban residencies. 37.5% of injuries were due to falls and 31.7% of children were involved as passengers or pedestrians in motor vehicle accidents. CT and MRI data was collected for 85.6% patients, of which 82% showed abnormalities.
Table 1. Patient demographics of children with moderate to severe acquired brain injury.† † Note that information is only reported for those cases where it was available. Undefined cases are cases that were clinically moderate to severe but GCS and PTA were not clearly recorded.
Outcomes
Neuropsychological deficit (Table 2)
Sex and age at onset were not associated with any significant differences in neuropsychological outcomes. As expected, severe ABI has a trend towards more deficits as compared to moderate ABI. Children often had deficits in more than one domain, and children with severe injuries had higher rates of reported deficits. Almost all cases of children who had no deficits on neuropsychological testing were children with moderate ABI. Over time, there was improvement in the numbers of children with reported deficits across attention, memory, information processing, and executive functioning. There was no increase in incidence of deficits over time. Many children with deficits recorded at 0-6 months recovered by 18 or 30 months of follow-up.
Table 2. Number of children with moderate to severe acquired brain injury with neuropsychological deficits at follow up. †Non-traumatic cases had consequences considered to reflect moderate to severe ABI but there was insufficient information on GCS for status to be clearly defined. Note that information is only reported for those cases where it was available. This table therefore does not report on the entire sample of 104. Undefined cases are cases that were clinically moderate to severe but GCS and PTA were not clearly recorded.
Co-morbidities
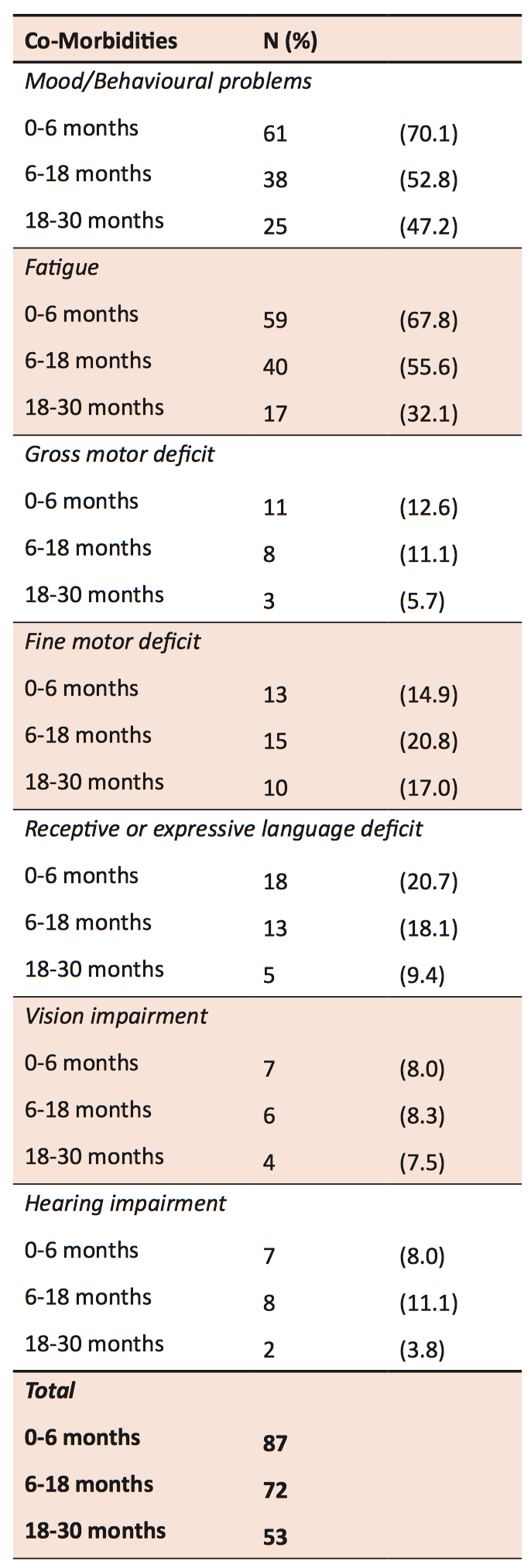
The most common complaints reported were headache, fatigue, and dizziness. From 0-6 months, 62 children reported fatigue. Mood and behavioural problems were also common, with 61 children reporting problems between 0-6 months, 38 at 6-18 months, and 25 at 18-30 months. Persistence of mood and behavioural problems discussed by parents and children at rehabilitation clinics even two-and-a-half years after injury reflects the ongoing difficulties faced by children with ABI even after physical injuries have healed.
Fine motor deficits were slightly more common than gross motor deficits. For gross motor deficits, from 0-6 months, there were a greater number of children with impaired mobility requiring aid, than those without aide, but between 6-30 months, the majority of children with impaired mobility were able to walk without an aide. Over a fifth of children had initial reports from brain injury clinic reviews describing receptive or expressive language problems, but two thirds of these were resolved by 30 months follow-up. Between 2-8% of children experienced vision or hearing problems after ABI. Except for fine motor deficits, co-morbidities were most frequently recorded during the first 6 months. The frequencies of co-morbidities were recorded at each of the follow-up time points (Table 3).
Table 3. Frequency of co-morbidities reported for children with moderate to severe ABI at follow-up.† †Note that information is only reported for those cases where it was available for all co-morbidities. This table therefore does not report on the entire sample of 104.
School attendance
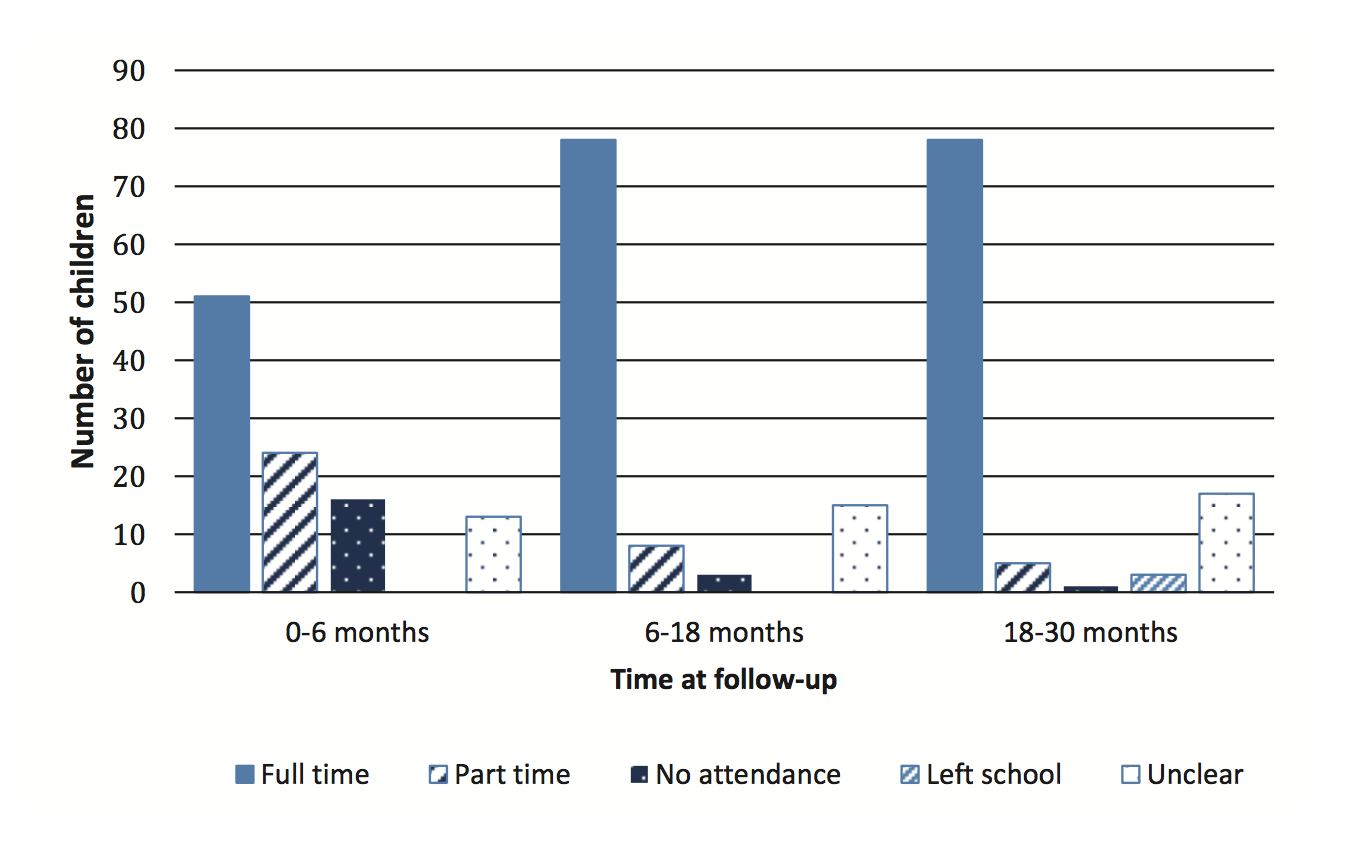
Attendance improved over time; most part-time students transitioned into full-time schooling by 18 months (Figure 1). At the end of 18-30 months follow up, 6.9% (n = 87) remained unable to return to full-time schooling.
Figure 1. School attendance for 104 children with moderate to severe brain injury over follow up.
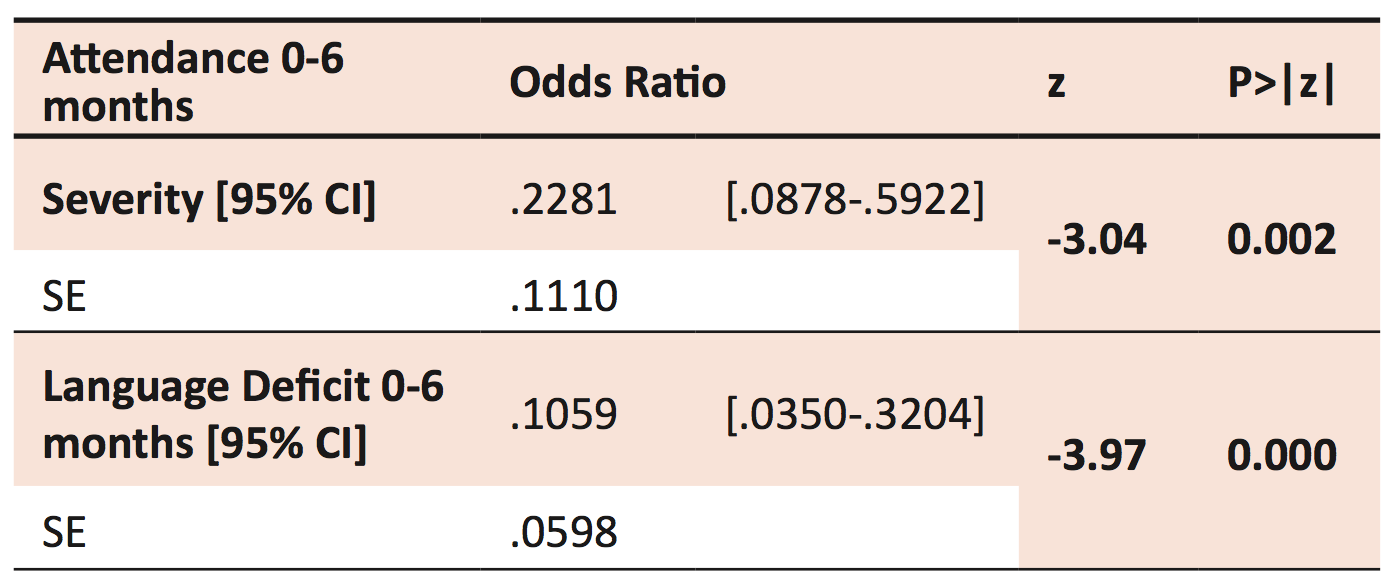
Ordered logistic regression was performed to identify predictors of school attendance. As expected, injury severity was negatively associated with full-time school attendance at 0-6 months post-injury. A child with severe ABI was five times less likely to attend school within six months post-injury than a child with moderate ABI (Table 4). There was a significant difference in school attendance at 18 months post-injury for children with moderate versus severe injury (p < 0.05). No relationship was found at 30 months (p > 0.2). No significant statistical impact of individual neuropsychological measures and attendance of schooling was found.
Table 4. Ordered logistical regression of attendance 0-6 months for 63 children with moderate to severe ABI.† †SE= Standard Error. Likelihood Ratio chi2(2) = 24.58 Prob > chi2 = 0.0000 Log likelihood = -52.060058 Pseudo R2= 0.191
Of the co-morbidities measured, it was found that injury severity and language deficit (independently and in combination) were negatively associated with full-time school attendance at 0-6 months post-injury. A child with a receptive or expressive language deficit was ten times less likely to attend school within six months post-injury than a child without a known language deficit.
School aide and change of school
Classroom aide was received by 3.3% of children at 0-6 months follow-up, by 12.8% at 6-18 months, and by 13.4% at 18-30 months. There was a significant difference according to injury severity for provision of a teaching aide at 18-30 months (p < 0.03). Special classes or educational programs were provided for 1.1% of children at 0-6 months follow-up, by 5.3% at 6-18 months, and by 7.2% at 18-30 months. There was some overlap with children receiving both aide assistance and attending a special class. During follow-up, seven children required a change of school for reasons relating to their ABI. Of these children, five had experienced severe ABI.
Discussion
This study describes the pattern of children in accessing schooling and special education or aide support following ABI. Extended absences from school are one of the initial challenges facing children after ABI; 17.6% of children in our study population did not attend school in the first six months post-ABI. Whilst hospital and home schooling were sometimes available, this represents a considerable time difference in which children with ABI may fall behind their peers. This study found that a combination of severity of injury and language deficit were found to be predictive of attendance in the first six months after injury. The involvement of language as a predictive factor is important, as it is modifiable. Language is important to complex learning and adaptation and contributes to understanding shared meanings in contexts such as school [18,19]. Language intervention programs may be able to facilitate earlier transition back to school. This study shows that the great majority (93%) of children with moderate or severe ABI will be able to return to full-time schooling. It also shows that the majority of these children are not given provision of classroom aides, special classes, or educational programs.
Attention to classroom instructions, reasoning and expression of ideas, and self-monitoring are all important features of good reintegration to schooling [20]. Children with severe ABI accounted for a greater proportion of neurological deficits in every domain measured (intellect, attention, memory, executive function, and information processing), and 44 of the 45 children with no reported neuropsychological deficits on testing had only moderate ABI. Our study reinforces that there is great variability in the way that ABI affects children, but severe ABI generally has a poorer prognosis and such children may experience greater challenges when returning to school. It is reassuring to note that time can help reduce the burden of ABI, with prevalence of neuropsychological deficits generally improving during follow-up. Longer-term studies suggest that intellect and personality problems may resolve by adulthood, but that reduced quality of life in relation to education and employment can persist [1]. Further long-term follow-up of these patients may be valuable in investigating this. Our study also found that attendance also improves with time, as 89.7% of children were able to resume full-time schooling by 30 months post-injury.
The presence of a classroom aide and modified learning programs is important in exploring whether the ongoing needs of children with ABI are met by schools. Our study found that 13% were provided with classroom aide during 30 months of follow-up. The provision of aid was found to increase over time. This may be accounted for by the inability of children with severe injuries to return to school early but another possible explanation is that there is a delay in the processing and provision of aid.
Quality of aide provision and the satisfaction children and their families had with the schooling system were not measured in this study. This is a possible avenue for future research, as general school educators and also special education teachers often do not have specialised training for working with children with ABI. TBI Consulting Team and BrainSTARS are two promising models currently available for improving professional development of educators in caring for children with ABI, but both require further studies to show objective improvement [21].
In our study, some children reported needing to repeat a year of school. Grade repetition is known to be a de-motivating process that can affect homework completion and predict greater amounts of school absence [22]. A possible direction for future research would be to examine how common grade repetition is amongst the ABI population.
Strengths and limitations of this study
This study addresses the need for a better understanding of educational outcomes for children with moderate to severe ABI. The follow-up time of 30 months also provides a clearer understanding of how outcomes change over time. Additionally, this study deals specifically with school attendance and provision of aide time, two outcomes which are often overlooked in studies describing participation of children in the community following ABI.
The study also provides important information regarding predictors of attendance in the first six months of schooling. Whilst severity has been a known predictor, language has not been a focus for research previously. This new information may help guide health and education professionals in providing appropriate resources to ensure the best educational outcomes for children with ABI [23].
This study had a number of methodical limitations. Due to the highly variable nature of ABI and the small sample size, subgroup analysis was limited. As the study was retrospective there were a number of missing data fields. The results may underestimate true incidence of neuropsychological deficits as standard clinical practice does not comprehensively test children at all points of follow-up if no changes are expected or testing is not necessary. A larger, prospective study of educational outcomes would provide more data for studies with larger patient cohorts to be undertaken in order to confirm our results [24].
The study did not include a control group so confounders were minimised by excluding children with previous intellectual deficits, moderate to severe brain injury, schooling problems, or behavioural difficulties.
This study was unable to detect differences for children who were previously above average, but dropped into an average category on neuropsychological testing. Unfortunately, pre-morbid capabilities are difficult to quantify without formal testing. This study would not consider these children to have a deficit even though they have experienced a change in abilities. Any changes in abilities should not be discounted as they can still negatively impact the expectations and lifestyle of children and their families.
Conclusion
Children with moderate to severe ABI experience a wide range of neuropsychological and physical co-morbidities that can persist for at least 30 months following injury. Greater severity of injury and presence of language deficit are predictive of school attendance of children in the first six months following ABI. 13% of children required additional aide support or involvement in special classes. Over a third of children still reported fatigue and behavioural problems at 30 months follow-up. This study shows that whilst patients and families experience a long and difficult process of recovery, they may be able to expect improvements over time, and children are very likely to have returned to full-time schooling by 30 months post-injury.
Acknowledgements
I would like to thank Dr Angela Morrow for her supervision and guidance throughout this research project. I would further wish to express my gratitude to Dr Barzi for great assistance with the statistics and to Julie-Anne Macey, who came up with the research concept. I would also like to thank Dr Patrina Caldwell for her encouragement and invaluable feedback during the editing process.
References
[1] Anderson V, Brown S, Newitt H, Hoile H. Long-term outcome from childhood traumatic brain injury: intellectual ability, personality, and quality of life. Neuropsychology. 2011;25(2):176-84.
[2] Anderson V, Le Brocque R, Iselin G, Eren S, Dob R et al. Adaptive ability, behavior and quality of life pre and posttraumatic brain injury in childhood. Disabil Rehabil. 2012.
[3] Aitken ME, Mele N, Barrett KW. Recovery of injured children: parent perspectives on family needs. Arch Phys Med Rehab. 2004;85(4):567-73.
[4] Catalano RF, Oesterle S, Fleming CB, Hawkins JD. The importance of bonding to school for healthy development: findings from the social development research group. J School Health. 2004;74(7):252-61.
[5] Beaulieu CL. Rehabilitation and outcome following pediatric traumatic brain injury. The Surgical Clinics of North America. 2002;82(2):393-408.
[6] Stewart-Scott AM, Douglas JM. Educational outcome for secondary and postsecondary students following traumatic brain injury. Brain Injury. 1998;12(4):317-31.
[7] Sharp NL, Bye RA, Llewellyn GM, Cusick A. Fitting back in: adolescents returning to school after severe acquired brain injury. Disabil Rehabil. 2006;28(12):767-78.
[8] Galvin J, Froude EH, McAleer J. Children’s participation in home, school and community life after acquired brain injury. Aust Occup Ther J. 2010;57(2):118-26.
[9] Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Functional plasticity or vulnerability after early brain injury? Pediatrics. 2005;116(6):1374-82.
[10] Anderson VA, Catroppa C, Haritou F, Morse S, Rosenfeld JV. Identifying factors contributing to child and family outcome 30 months after traumatic brain injury in children. J Neurol Neurosur PS. 2005;76(3):401-8.
[11] Catroppa C, Anderson VA, Morse SA, Haritou F, Rosenfeld JV. Outcome and predictors of functional recovery 5 years following pediatric traumatic brain injury (TBI). J Pediatr Psychol. 2008;33(7):707-18.
[12] Catroppa C, Anderson V. Recovery in memory function, and its relationship to academic success, at 24 months following pediatric TBI. Child Neuropsychol. 2007 May; 13(3):240-61.
[13] Miller LJ, Donders J. Prediction of educational outcome after pediatric traumatic brain injury. Rehabil Psychol. 2003;48:237–241
[14] Neuroimaging. 2012;22(2):e1-e17.
Arnett AB, Peterson RL, Kirkwood MW, Taylor HG, Stancin T et al, Behavioral and cognitive predictors of educational outcomes in pediatric traumatic brain injury. J Int Neuropsychol Soc. 2013;19(8):881-9.
[15] Pinto PS, Poretti A, Meoded A, Tekes A, Huisman TA. The unique features of traumatic brain injury in children. Review of the characteristics of the pediatric skull and brain, mechanisms of trauma, patterns of injury, complications and their imaging findings–part 1. J Neuroimaging. 2012;22(2):e1-e17.
[16] Welfare AIoHa. Disability in Australia: trends in prevalence, education, employment and community living. Canberra: AIHW, 2008.
[17] Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81-4.
[18] Marlowe WB. An intervention for children with disorders of executive functions. Dev Neuropsychol. 2000;18(3):445-54.
[19] Ewing-Cobbs L, Barnes M. Linguistic outcomes following traumatic brain injury in children. Semin Pediat Neurol. 2002;9(3):209-17.
[20] Semrud-Clikeman M. Pediatric Traumatic Brain injury: rehabilitation and transition to home and school. Appl Neuropsychol. 2010;17(2):116-22.
[21] Glang A, Todis B, Sublette P, Brown BE, Vaccaro M. Professional development in TBI for educators: the importance of context. J Head Trauma Rehab. 2010;25(6):426-32.
[22] Martin AJ. Holding back and holding behind: grade retention and students’ non-academic and academic outcomes. Brit Educ Res J. 2010;37(5):739-63.
[23] Hawley CA, Ward AB, Magnay AR, Mychalkiw W. Return to school after brain injury. Arch Dis Child. 2004;89(2):136-42.
[24] Slomine B, Locascio G. Cognitive rehabilitation for children with acquired brain injury. Dev Disabil Res Rev. 2009;15(2):133-43.
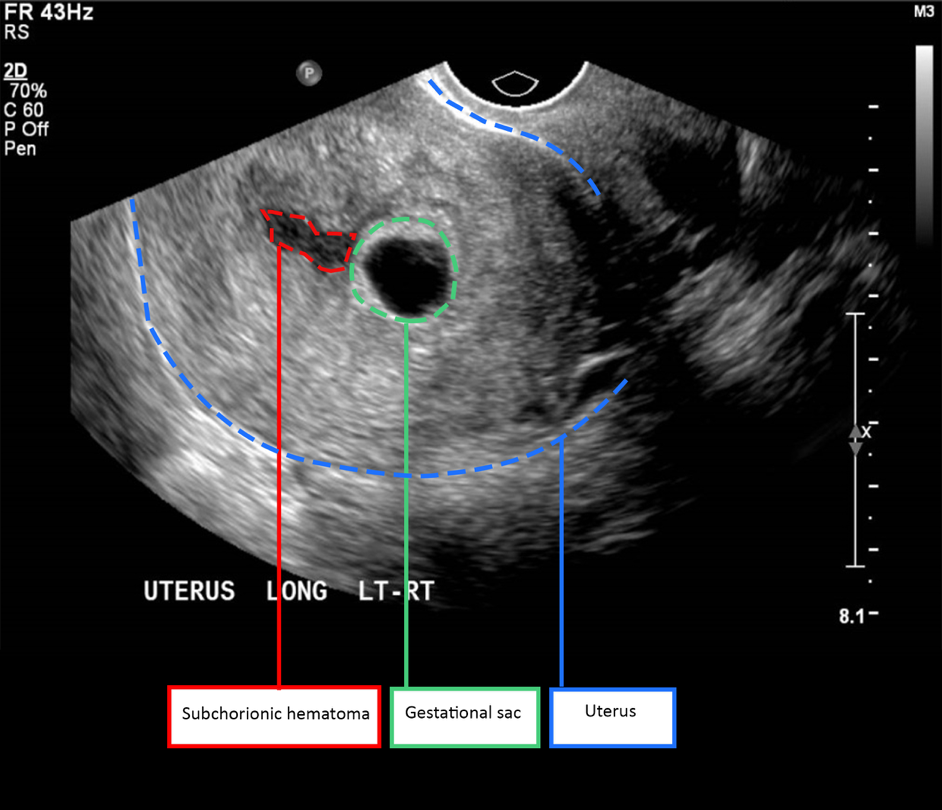
Introduction: Subchorionic haematoma (SCH) is the most common ultrasound abnormality found in women with symptoms of threatened miscarriage. It refers to a collection of blood between the chorionic membrane and the uterine wall. Depending on the time the haematoma is formed, it may appear as either hypoechoic or hyperechoic on the ultrasound. The cause of SCH may be related to poor placentation. Although SCH is common, the effects of SCH on pregnancy outcomes are unclear. The review aims to provide an overview of the effects of SCH on pregnancy outcomes and identify prognostic factors that may predict adverse pregnancy outcomes in women with SCH.
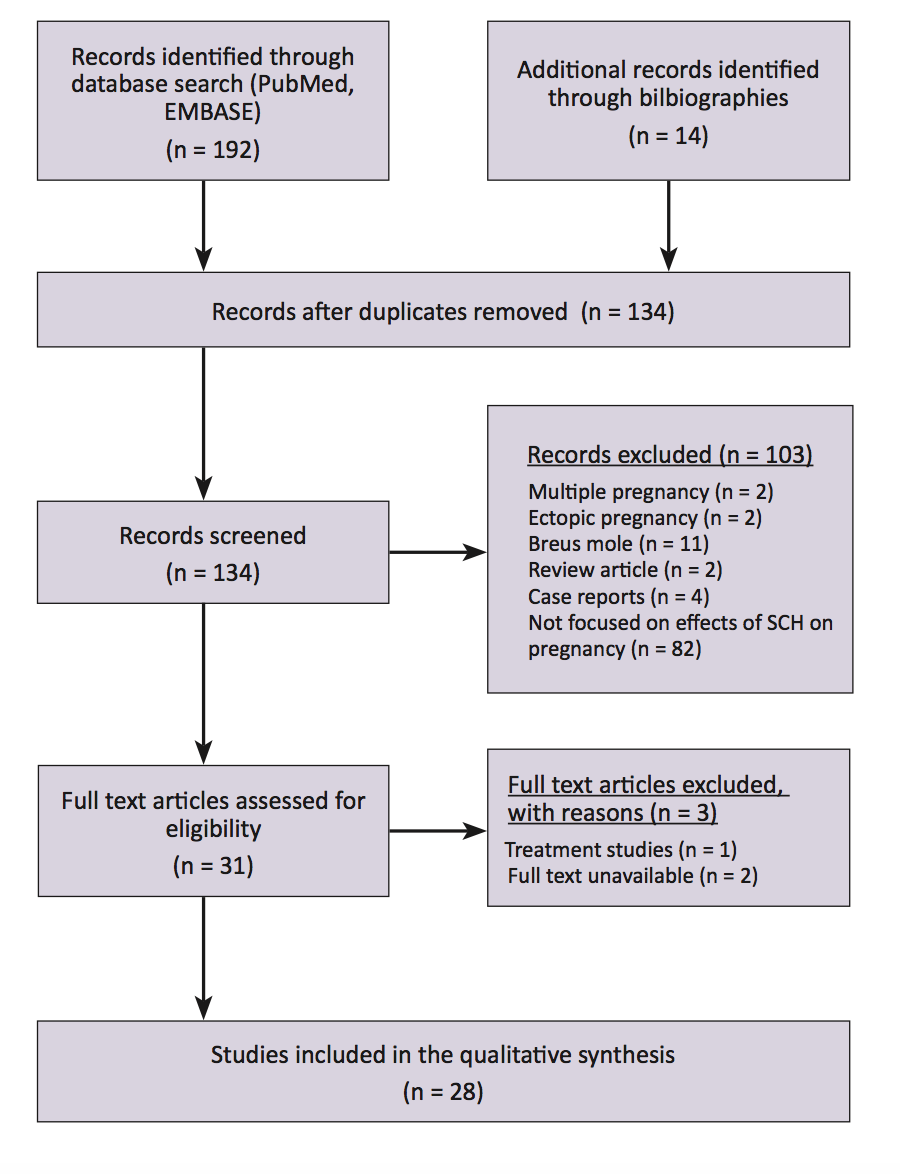
Methods: To identify the relevant literature, electronic databases (PubMed and EMBASE) were searched using the search terms: “subchorionic haematoma” and “subchorionic hemorrhage”. Exclusion criteria include multiple pregnancy, ectopic pregnancy, Breus mole, review articles, case reports, and studies that did not focus on the effects of SCH on pregnancy outcomes.
Results and conclusion: Women with SCH have an increased risk of placental abruption. Studies are conflicting on the risk SCH poses on pregnancy loss. There are only limited studies on other adverse pregnancy outcomes such as preterm delivery, small for gestational age, pre-eclampsia, and chorioamnionitis. Factors that may predict an increased likelihood of adverse pregnancy outcomes in SCH include: large haematoma size, fundal or retroplacental location, early gestational age of diagnosis (before 9 weeks), and severity of symptoms. Persistent SCH is rare but it carries a high risk of complications, including chorioamnionitis.
Introduction
Up to 25% of pregnant women experience symptoms of threatened miscarriage, namely first trimester per vaginum (PV) bleeding with or without uterine contractions [1]. The most common ultrasound abnormality in these women is a subchorionic haematoma (SCH) [2]. SCH is a collection of blood between the chorionic membrane and the uterine wall [2]. Typically, it appears as a crescenteric hypoechoic lesion around the gestational sac [2]. According to a 2014 retrospective cohort study from Turkey, the reported incidence of SCH in women with symptoms of threatened abortion is 18.2% [3]. In the general obstetric population, the incidence of SCH varies between 1.7% to 3.1% [4,5].
Pathophysiology
The exact pathophysiology of SCH is still unknown. Nevertheless, the underlying cause of SCH is believed to be poor placentation [3,6]. Poor placentation can impair angiogenesis and lead to the formation of weak vessels that tear easily [3,6]. In SCH, it is postulated that the marginal utero-placental veins tear and cause low pressure bleeding [7]. The blood then tracks around the gestational sac to form a cresenteric haematoma between the chorionic membrane and the uterine wall [7]. In contrast, the bleeding in placental abruption is usually high pressure bleeding from ruptured spiral arterioles [8]. Results from a recent Japanese study appear to support the theory that SCH is caused by poor placentation [9]. The study found that SCH is more common in women with risk factors for poor placentation such as multiparity and pregnancies conceived through in-vitro fertilisation, especially those using a frozen-thawed embryo transfer [9].
Clinical presentation
While some SCH are asymptomatic, most can present with first trimester PV bleeding with or without uterine contractions [5,10]. In most cases (up to 70%), PV bleeding of varying degree, ranging from spotting to heavy bleeds, can continue intermittently for 1 – 3 months after the diagnosis of SCH [11]. The symptoms usually resolve spontaneously during the second trimester [11]. However, a small minority of women (0.46% of all obstetric patients) can have a persistent SCH that remains symptomatic until delivery [11].
Diagnosis
SCH is diagnosed using ultrasound (Figure 1). The characteristic sonographic finding is a hypoechoic cresenteric lesion between the chorionic membrane and the uterine wall [2]. The haematoma may appear hyperechoic initially but with time, it becomes hypoechoic [2]. Possible differential diagnoses for this sonographic finding include chorioamniotic separation and twin gestational sac [2].
Figure 1. First trimester subchorionic haematoma.
Rationale and aims
Although SCH is very common in women with symptoms of threatened miscarriage, the effects of SCH on pregnancy outcomes are unclear. This review aims to provide an overview of the effects of SCH on pregnancy outcomes. It also aims to identify prognostic factors that may predict adverse pregnancy outcomes in women with SCH.
Methods
To identify the relevant literature, electronic databases (PubMed and EMBASE) were searched using the search terms: subchorionic haematoma and subchorionic hemorrhage. The search was limited to English-language human studies published between January 1981 and June 2016. A total of 192 studies were identified from the database search and an additional 14 studies were identified from manual review of bibliographies. After removing the duplicates, studies were excluded for reasons such as multiple pregnancy (n = 2), ectopic pregnancy (n = 2), Breus mole (n = 11), review articles (n = 2), case reports (n = 4) and different study focus (n = 82) (Figure 2). For this review, 28 studies discussing the effects of SCH on pregnancy outcomes were included.
Figure 2. PRISMA study flow diagram.
Effects on pregnancy outcomes
Adverse pregnancy outcomes that may be associated with SCH include early and late pregnancy loss, placental abruption, preterm delivery (PTD), preterm premature rupture of membrane (pPROM), small for gestational age (SGA) and chorioamnionitis. The pathophysiological mechanisms behind how SCH might contribute to these adverse pregnancy outcomes remains unclear. It is thought that SCH may cause pregnancy loss through either a direct mechanical effect or an indirect inflammatory response [12]. As for placental abruption, studies suggest that the underlying cause of SCH – poor placentation – also predisposes the patients to placental abruption [5,13].
Early and late pregnancy loss
In several studies, SCH is associated with an increased risk of miscarriage (pregnancy loss before 20 weeks) and stillbirth (pregnancy loss after 20 weeks). In a recent study, Sukur et al. [3] reported that the miscarriage rate was significantly higher in women with SCH compared to those without (29.5% versus 12.6%). A similar finding was obtained by Kurjak et al. [14]. According to Ozkaya et al. [15], the risk of miscarriage was six times higher in women with SCH (OR = 6.29, 95% CI 1.43 – 37.7). In a separate study, the risk of miscarriage remained significantly higher in cases of SCH even after PV bleeding has stopped [16]. Stillbirths are also more common in women with SCH compared to women without SCH [13]. Ball et al. [13] found that the risk of stillbirth was significant when compared to women both with and without PV bleeding. From a meta-analysis performed in 2011, SCH doubled the risk of miscarriage and stillbirth (OR = 2.18, 95% CI 1.29 – 3.68 and OR = 2.09, 95% CI 1.20 – 3.67, respectively) [6]. Based on the meta-analysis, for every 11 women with SCH, there was one additional miscarriage [6].
However, some studies had contrasting results. Two small studies (n = 22, n = 62) of SCH did not find that SCH increases the miscarriage rate [17,18]. In one of these studies, there were no miscarriages in all 22 cases of SCH studied [17]. Tower and Regan [19] studied the effect of SCH in a population with recurrent miscarriages. They found that SCH did not increase the miscarriage rate for these patients [19]. Based on a 2003 prospective study, women with SCH also did not have a significantly higher risk of stillbirth [5]. In a large retrospective study, the risk of stillbirth in women with SCH was not significant after adjusting for ethnicities, PV bleeding, chronic hypertension, pregestational diabetes, and smoking [4].
The mixed results from different studies suggest that the effect of SCH on pregnancy loss is complicated. Not all cases of SCH have an equal risk of miscarriage and stillbirth. The likelihood of pregnancy loss in SCH may depend on several prognostic factors, such as the size and location of haematoma.
Placental abruption
Unlike the risk of pregnancy loss, the risk of placental abruption in women with SCH is well established. When SCH is present, the risk of placental abruption increases from 0.6% to 3.6% (aOR = 2.6, 95% CI 1.8 – 3.7) [4]. This finding is echoed by several other studies [5,13,20]. From a meta-analysis that pooled together the results of four different studies, SCH increased the risk of placental abruption by more than fivefold (OR = 5.70, 95% CI 3.91 – 8.33) [6]. The number needed to harm was only 34 [6]. Given that studies have consistently reported that women with SCH have a higher risk of placental abruption, SCH most likely has a true effect on the risk of placental abruption.
Preterm delivery (PTD)
Studies also found that women with SCH have a significantly higher risk of PTD [4,5,20,21]. In 2003, Nagy et al. [5] reported that SCH doubled the risk of PTD (RR = 2.3, 95% CI 1.6 – 3.2). In their study, 43% of these PTD cases occurred before 34 weeks and 10% occurred before 28 weeks [5]. This result was corroborated by a large retrospective cohort study from 2010, which included more than 1000 cases of SCH [4]. More recently, Palatnik and Grobman [20] carried out a multivariable regression analysis and showed that SCH increased the risk of PTD independent of mid-trimester cervical length. There were several studies that did not find a correlation between SCH and preterm delivery [3,13,14,18,19]. However, these studies were smaller in size, with only one of the studies having more than 100 cases of SCH [13]. Nevertheless, more studies are required to confirm the risk of PTD in women with SCH.
Chorioamnionitis
Chorioamnionitis is a rare but severe complication in pregnancy that can cause life-threatening neonatal sepsis. Currently, the risk of chorioamnionitis in women with SCH is still unknown. There was only one study that extensively investigated the risk of chorioamnionitis in SCH [11]. In that study, Seki et al. [11] reported that chorioamnionitis was particularly common amongst women with persistent SCH. Six out of 22 women (27.3%) with persistent SCH had chorioamnionitis [11]. Half of these women had a miscarriage, while the other half delivered preterm [11]. In the study, persistent SCH was defined as a haematoma with clinical symptoms that lasted until delivery [11]. Recently, a study found that women with SCH had significantly different vaginal swab culture results [22]. Women with SCH had significantly higher prevalence of coagulase-negative Staphylococcus and Gardnerella vaginalis and lower prevalence of Lactobacillus on vaginal swabs [22]. The culture result is suggestive, though not diagnostic of bacterial vaginosis, a condition that has been associated with chorioamnionitis, pPROM, and PTD [22]. However, in that study, the swabs were only collected in the second trimester, which was temporally distant from the time SCH was diagnosed [22]. Hence, a direct cause and effect relationship could not be confirmed through the study [22]. The risk of chorioamnionitis in women with SCH warrants further investigation.
Small for gestational age (SGA) and pre-eclampsia
Given that SCH may be associated with poor placentation, it is important to also consider other adverse pregnancy outcomes typically associated with poor placentation such as SGA and pre-eclampsia. SCH was associated with a significantly higher risk of SGA in two studies [5,15] and and pre-eclampsia in one study [5]. However, the majority of the studies did not support a significant relationship between SCH and SGA [3,4,12,13,19,20]. SCH was also not associated with pre-eclampsia in multiple studies [4,12,19,20]. More importantly, in the two largest controlled studies on SCH (n = 512 and n = 1,081), SCH did not increase the risk of SGA or pre-eclampsia [4,20].
Preterm premature rupture of membrane (pPROM)
Limited studies recorded the incidence of pPROM in women with SCH. In a study by Palatnik and Grobman [20], pPROM was significantly more common in women with SCH compared to women without SCH (6.4% versus 4.0%). However, this finding was not reciprocated in two other studies [4,12].
Other adverse pregnancy outcomes
Interestingly, Nagy et al. [5] noted that women with SCH had significantly higher rates of an abnormally adherent placenta that required manual removal (13.9% versus 4.9%). Previously, two uncontrolled studies also noted that manual placenta removal was required in 7% and 11.1% of women with SCH [10, 23]. More controlled studies are needed to provide information about the risk.
Prognostic predictors
The likelihood of adverse pregnancy outcomes in SCH may depend on several prognostic factors. Differences in the size, location, and persistency of SCH, as well as, the gestational age of diagnosis and the severity of symptoms can all change how SCH affects pregnancy [24]. Examining these factors in closer detail can help clinicians clarify the risk of SCH.
Size of haematoma
The risk of adverse outcomes may be increased with larger haematoma size. In the original case series on SCH, Mantoni and Pederson [25] noted that SCH > 50mL occurring after 16 weeks gestation increased the risk of spontaneous abortion and PTD but SCH < 35 mL had a good prognosis. In one study, all women had SCH < 16 mL and none of them had a miscarriage [17]. In contrast, another study found that 81% of the pregnancies with SCH > 60 mL did not continue to term [21]. The rate of miscarriage appeared to be vastly different depending on the size of the SCH. Ozkaya et al. [15] used a receiver operating characteristic curve analysis (ROC) and determined that haematoma > 32 mL was 81% sensitive and 80% specific for predicting the risk of miscarriage. The size of haematoma was also shown to be an important factor for miscarriage in several other studies [23,26-29]. However, many studies did not observe an association between size and pregnancy loss [1,13,14,16,18,30,31]. Predicting the risk of miscarriage with the size of haematoma is controversial because of the mixed evidence. It has been suggested that size is not the best indicator of the extent of subchorionic bleeding [24]. This is because a larger haematoma can be caused by either an increase in subchorionic bleeding and a decrease in cervical drainage as PV bleeding [24]. This may explain why several studies did not find the size to be predictive of poor prognosis. While size may not correlate linearly with increased risk of miscarriage, haematoma above a certain volume may still confer a higher risk. This is because regardless of the cause, a larger haematoma can have more direct pressure-volume effect on the pregnancy. A significantly larger haematoma may also have greater placental involvement. Currently, the size of haematoma remains a controversial predictor of poor outcome.
Location of haematoma
Haematomas in certain locations may have a worse prognosis. Most SCH are located on the anterior aspect of the uterus and at the peripheries of the placenta [5,17]. Haematomas that were retroplacental or fundal had significantly higher rates of pregnancy loss according to several studies [14,29,30]. A fundal haematoma was four times more likely to cause a miscarriage compared to supra-cervical haematoma (27.5% versus 6.6%) [14]. While retroplacental location was a significant risk factor, Nyberg et al. [29] found that ultimately, it was the degree of placental involvement that best predicted foetal mortality. Using a multiple logistic regression analysis, Nyberg et al. [29] showed that the location was no longer significantly associated with foetal mortality after adjusting for placental involvement. Without any placental involvement, foetal mortality was only 8% [29]. When 20 – 50% of the placenta was involved, foetal mortality climbed to 20%. Greater than 50% of placental involvement resulted in a 75% foetal mortality rate [29]. Based on the current evidence, greater placental involvement and retroplacental or fundal location of haematoma may all be important risk factors for the poorer prognosis amongst women with SCH.
Persistency of haematoma
Most SCH will self-resolve in the second trimester but some can remain symptomatic until the delivery. This persistent SCH is rare and was only present in 0.46% of the general obstetric population [11]. Persistent SCH may carry a worse prognosis. Seki et al. [11] studied 22 cases of persistent SCH and found that while the miscarriage rate was not particularly high (13.6%), most women with persistent SCH experienced preterm labor (77.3%), half of which occurred before 32 weeks. There was also a high prevalence of chorioamnionitis amongst women with persistent SCH (27.3%) [11]. Aoki et al. also found that there is a higher rate of complications, including PTD, SGA, and neonatal lung disease in ten cases of persistent SCH [32]. Although there were no other studies on haematoma that persisted until delivery, several studies observed that haematoma that was slow to resolve or was associated with prolonged PV bleeding had higher rates of pregnancy loss [1,10,23,27]. The evidence is limited but persistent SCH appears to be associated with higher complication rates.
Gestational age of diagnosis
An earlier gestational age of diagnosis of SCH has been found to be a risk factor for worse outcomes in several studies. From a 2005 observational study, SCH diagnosed before 9 weeks has a significantly higher risk of pregnancy loss and an adverse outcome compared to SCH diagnosed after 9 weeks (aOR = 18.29, 95% CI 2.36 – 41.46 and aOR = 2.22, 95% CI 1.13 – 4.40, respectively), even after adjusting for other factors such as haematoma size and maternal age [33]. The study also showed that the risk of pregnancy loss increased from less than 2% to 20%, if the diagnosis occurred before 9 weeks [33]. Similar results were obtained by Bennett et al. [26]. However, the studies were not clear on when the symptoms of PV bleeding occurred in relation to the diagnosis of SCH. Furthermore, many other studies did not agree that an earlier gestational age of diagnosis was a significant prognostic factor [16,27,29,34]. In one study, an earlier gestational age of diagnosis was strongly associated with preterm labor but not pregnancy loss [29]. Yet, according to a 2003 study, there was no significant correlation between gestational age of diagnosis and risk of PTD [34]. Based on the current evidence, gestational age of diagnosis is not a clear risk factor for worse outcomes. A probable mechanism on how an earlier gestational age of diagnosis leads to adverse outcomes is also lacking in the existing studies.
Severity of symptoms
Asymptomatic SCH are common and benign [13,23,35]. In women with SCH, those that experienced PV bleeding were more likely to have PTD than those who were asymptomatic (OR = 4.8, 95% CI 1.2 – 15.9) [34]. Based on a study by Abu-Yousef et al. [27], most women (83%) with moderate-to-heavy PV bleeding had an unfavorable outcome. In contrast, most women (75%) with light PV bleeding had a favorable outcome [27]. The risk of an adverse pregnancy outcome is higher with more severe symptoms in SCH.
Management
Despite the effects SCH might have on pregnancy, there is no specific management guideline for SCH. This is partly because there are only limited studies on how to manage SCH. Currently, most women with SCH are regularly monitored using ultrasound until the haematoma resolves. Otherwise, women with SCH are managed similarly to other women with threatened miscarriage, with advice on bed rest and supplementary progestogen. However, bed rest is not considered to be beneficial for women with threatened miscarriage based on the results of a Cochrane review [36]. There was one non-randomised controlled trial that showed a lower miscarriage rate in women with SCH that had bed rest (6.5% versus 23.3%) [37]. However, given that the study lacked randomisation and was performed retrospectively, the evidence is weak and inconclusive. In terms of progestogen, a Cochrane review of four randomised controlled trials found that it reduced the rate of spontaneous abortion in women with threatened miscarriage significantly (RR = 0.53, 95% CI 0.35 – 0.79) [38]. The beneficial effects of progestogen may be related to its immunomodulatory properties. Progestogen increases the production of progesterone-induced blocking factor, which favors T-helper cell type 2 response [39-41]. Besides that, progestogen may also help by promoting implantation and inhibiting uterine contraction and cervical dilation [39,41]. In several trials, progestogen was beneficial for women with SCH [40,41]. Pandian reported that dydrogesterone given as 40 mg/day stat. followed by 10 mg twice daily until 16 weeks gestation reduced the miscarriage rate by 15.9% (OR = 0.36, 95% CI 0.172 – 0.756) [41]. In another study, taking 40 mg of oral dydrogesterone daily until 16 weeks gestation resulted in maintenance of pregnancies for 93% of women with SCH [40]. Although the results are encouraging, more studies are needed to confirm the benefits of progestogen. Patients and clinicians should weigh the cost and benefits carefully, before starting on progestogen treatment.
A novel drug, called vaginal alpha lipoic acid (ALA), is currently being investigated for its potential use in SCH management [42]. A randomised controlled trial has shown that women taking 10 mg of vaginal ALA had faster resorption of SCH compared to women taking 400 mg progesterone and women without any medication [42]. ALA is thought to be beneficial because of its immunomodulatory properties [42]. However, the trial was a small pilot study with only 76 patients [42]. It is not powered to detect a change in the clinical outcome of miscarriage rate (3/27 in ALA group and 6/27 in progesterone group) [42]. It is still unclear whether faster resorption of SCH would improve clinical outcomes.
Learning points for medical students
For women with symptoms of threatened miscarriage, SCH is the most common ultrasound abnormality detected. It has been suggested that the cause of SCH may be poor placentation, which leads to formation of weak marginal uteroplacental veins that tear and bleed. SCH significantly increases the risk of placental abruption but studies are still conflicting on whether it increases the risk of pregnancy loss and other adverse outcomes including PTD, SGA, pre-eclampsia, and chorioamnionitis. Predictors of poor outcomes include the size of haematoma, location with greater placental involvement, persistency of haematoma, earlier gestational age of diagnosis, and severity of symptoms. Management of SCH involves regular ultrasound monitoring. There are potential benefits with bed rest and supplementary progestogen in some studies but the evidence is still limited. Vaginal ALA is a novel treatment option that is still under investigation. In the future, larger controlled studies that measure all the various prognostic factors will help provide better information on the risk posed by SCH.
Acknowledgements
I would like to thank Dr. Shavi Fernando for his advice and the Monash Diagnostic Imaging Department for providing the ultrasound image of the subchorionic haematoma.
Conflicts of interest
None declared
References
[1] Goldstein SR, Subramanyam BR, Raghavendra BN, Horii SC, Hilton S. Subchorionic bleeding in threatened abortion: sonographic findings and significance. AJR Am J Roentgenol. 1983;141(5):975-8.
[2] Trop I, Levine D. Hemorrhage during pregnancy: sonography and MR imaging. AJR Am J Roentgenol. 2001;176(3):607-15.
[3] Sukur YE, Goc G, Kose O, Acmaz G, Ozmen B, Atabekoglu CS, et al. The effects of subchorionic hematoma on pregnancy outcome in patients with threatened abortion. Journal of the Turkish German Gynecological Association. 2014;15(4):239-42.
[4] Norman SM, Odibo AO, Macones GA, Dicke JM, Crane JP, Cahill AG. Ultrasound-detected subchorionic hemorrhage and the obstetric implications. Obstet Gynecol. 2010;116(2 Pt 1):311-5.
[5] Nagy S, Bush M, Stone J, Lapinski RH, Gardo S. Clinical significance of subchorionic and retroplacental hematomas detected in the first trimester of pregnancy. Obstet Gynecol. 2003;102(1):94-100.
[6] Tuuli MG, Norman SM, Odibo AO, Macones GA, Cahill AG. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet Gynecol. 2011;117(5):1205-12.
[7] Hertzberg BS, Middleton WD. Placenta, Umbilical cord, and cervix. Ultrasound: The Requisites. Third ed: Elsevier Health Sciences; 2015. p. 469-95.
[8] Goldstein C, Hagen-Ansert SL. First-trimester complications. Textbook of Diagnostic Sonography. Seventh ed: Mosby; 2011. p. 1081-102.
[9] Asato K, Mekaru K, Heshiki C, Sugiyama H, Kinjyo T, Masamoto H, et al. Subchorionic hematoma occurs more frequently in in vitro fertilization pregnancy. Eur J Obstet Gynecol Reprod Biol. 2014;181:41-4.
[10] Jouppila P. Clinical consequences after ultrasonic diagnosis of intrauterine hematoma in threatened abortion. J Clin Ultrasound. 1985;13(2):107-11.
[11] Seki H, Kuromaki K, Takeda S, Kinoshita K. Persistent subchorionic hematoma with clinical symptoms until delivery. Int J Gynaecol Obstet. 1998;63(2):123-8.
[12] Johns J, Hyett J, Jauniaux E. Obstetric outcome after threatened miscarriage with and without a hematoma on ultrasound. Obstet Gynecol. 2003;102(3):483-7.
[13] Ball RH, Ade CM, Schoenborn JA, Crane JP. The clinical significance of ultransonographically detected subchorionic hemorrhages. Am J Obstet Gynecol. 1996;174(3):996-1002.
[14] Kurjak A, Schulman H, Zudenigo D, Kupesic S, Kos M, Goldenberg M. Subchorionic hematomas in early pregnancy: clinical outcome and blood flow patterns. J Matern Fetal Med. 1996;5(1):41-4.
[15] Ozkaya E, Altay M, Gelisen O. Significance of subchorionic haemorrhage and pregnancy outcome in threatened miscarriage to predict miscarriage, pre-term labour and intrauterine growth restriction. J Obstet Gynaecol. 2011;31(3):210-2.
[16] Borlum KG, Thomsen A, Clausen I, Eriksen G. Long-term prognosis of pregnancies in women with intrauterine hematomas. Obstet Gynecol. 1989;74(2):231-3.
[17] Stabile I, Campbell S, Grudzinskas JG. Threatened miscarriage and intrauterine hematomas. Sonographic and biochemical studies. J Ultrasound Med. 1989;8(6):289-92.
[18] Pedersen JF, Mantoni M. Prevalence and significance of subchorionic hemorrhage in threatened abortion: a sonographic study. AJR Am J Roentgenol. 1990;154(3):535-7.
[19] Tower CL, Regan L. Intrauterine haematomas in a recurrent miscarriage population. Hum Reprod. 2001;16(9):2005-7.
[20] Palatnik A, Grobman WA. The relationship between first-trimester subchorionic hematoma, cervical length, and preterm birth. Am J Obstet Gynecol. 2015;213(3):403.e1-4.
[21] Sauerbrei EE, Pham DH. Placental abruption and subchorionic hemorrhage in the first half of pregnancy: US appearance and clinical outcome. Radiology. 1986;160(1):109-12.
[22] Yamada T, Atsuki Y, Wakasaya A, Kobayashi M, Hirano Y, Ohwada M. Characteristics of patients with subchorionic hematomas in the second trimester. J Obstet Gynaecol Res. 2012;38(1):180-4.
[23] Mandruzzato GP, D’Ottavio G, Rustico MA, Fontana A, Bogatti P. The intrauterine hematoma: diagnostic and clinical aspects. J Clin Ultrasound. 1989;17(7):503-10.
[24] Xiang L, Wei Z, Cao Y. Symptoms of an intrauterine hematoma associated with pregnancy complications: a systematic review. PLoS One. 2014;9(11):e111676.
[25] Mantoni M, Pedersen JF. Intrauterine haematoma. An ultrasonic study of threatened abortion. Br J Obstet Gynaecol. 1981;88(1):47-51.
[26] Bennett GL, Bromley B, Lieberman E, Benacerraf BR. Subchorionic hemorrhage in first-trimester pregnancies: prediction of pregnancy outcome with sonography. Radiology. 1996;200(3):803-6.
[27] Abu-Yousef MM, Bleicher JJ, Williamson RA, Weiner CP. Subchorionic hemorrhage: sonographic diagnosis and clinical significance. AJR Am J Roentgenol. 1987;149(4):737-40.
[28] Dongol A, Mool S, Tiwari P. Outcome of pregnancy complicated by threatened abortion. Kathmandu Univ Med J (KUMJ). 2011;9(33):41-4.
[29] Nyberg DA, Mack LA, Benedetti TJ, Cyr DR, Schuman WP. Placental abruption and placental hemorrhage: correlation of sonographic findings with fetal outcome. Radiology. 1987;164(2):357-61.
[30] Glavind K, Nohr S, Nielsen PH, Ipsen L. Intra-uterine hematoma in pregnancy. Eur J Obstet Gynecol Reprod Biol. 1991;40(1):7-10.
[31] Bloch C, Altchek A, Levy-Ravetch M. Sonography in early pregnancy: the significance of subchorionic hemorrhage. Mt Sinai J Med. 1989;56(4):290-2.
[32] Aoki S, Inagaki M, Kurasawa K, Okuda M, Takahashi T, Hirahara F. Retrospective study of pregnant women placed under expectant management for persistent hemorrhage. Arch Gynecol Obstet. 2014;289(2):307-11.
[33] Maso G, D’Ottavio G, De Seta F, Sartore A, Piccoli M, Mandruzzato G. First-trimester intrauterine hematoma and outcome of pregnancy. Obstet Gynecol. 2005;105(2):339-44.
[34] Sharma G, Kalish RB, Chasen ST. Prognostic factors associated with antenatal subchorionic echolucencies. Am J Obstet Gynecol. 2003;189(4):994-6.
[35] Dickey RP, Olar TT, Curole DN, Taylor SN, Matulich EM. Relationship of first-trimester subchorionic bleeding detected by color Doppler ultrasound to subchorionic fluid, clinical bleeding, and pregnancy outcome. Obstet Gynecol. 1992;80(3 Pt 1):415-20.
[36] Aleman A, Althabe F, Belizan J, Bergel E. Bed rest during pregnancy for preventing miscarriage. The Cochrane database of systematic reviews. 2005(2):Cd003576.
[37] Ben-Haroush A, Yogev Y, Mashiach R, Meizner I. Pregnancy outcome of threatened abortion with subchorionic hematoma: possible benefit of bed-rest? Isr Med Assoc J. 2003;5(6):422-4.
[38] Wahabi HA, Fayed AA, Esmaeil SA, Al Zeidan RA. Progestogen for treating threatened miscarriage. The Cochrane database of systematic reviews. 2011(12):Cd005943.
[39] Carp H. A systematic review of dydrogesterone for the treatment of threatened miscarriage. Gynecol Endocrinol. 2012;28(12):983-90.
[40] Pelinescu-Onciul D. Subchorionic hemorrhage treatment with dydrogesterone. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology. 2007;23 Suppl 1:77-81.
[41] Pandian RU. Dydrogesterone in threatened miscarriage: a Malaysian experience. Maturitas. 2009;65 Suppl 1:S47-50.
[42] Costantino M, Guaraldi C, Costantino D. Resolution of subchorionic hematoma and symptoms of threatened miscarriage using vaginal alpha lipoic acid or progesterone: clinical evidences. Eur Rev Med Pharmacol Sci. 2016;20(8):1656-63.
Aim: To ascertain the function of miRNA-34a in hepatocellular carcinoma (HCC) and to assess its use as a therapeutic agent through the analysis of pre-clinical and clinical trials.
Discussion: Multiple studies found that miRNA-34a was down-regulated in the majority of human HCC samples and subsequently had a tumour suppressor role via the inhibition of a number of target genes essential for carcinogenesis. MRX34, a miRNA-34a mimic, is currently in an ongoing phase I clinical trial. Interim data has indicated that this therapy has a manageable safety profile, with a partial response observed in one patient. The combination of miRNA-34a with other agents has also proven to exert enhanced anti-tumour effects. Conversely, many studies have reported that miRNA-34a was up-regulated in HCC samples, particularly in those with activation of the beta-catenin pathway.
Conclusion: Pre-clinical studies have shown promising results in the use of a miRNA-34a mimic in HCC as a single agent or as a combination therapy, however, the results from the phase I trial are yet to be fully established. The mechanisms of miRNA-34a in HCC remain to be elucidated, with further research required into its proposed oncogenic role, especially relating to the clinical implications of this interaction.
Introduction
Hepatocellular carcinoma (HCC) is the second most common cause of cancer-related deaths worldwide and is the most common form of liver cancer, accounting for between 85% and 90% of primary liver cancers [1]. The major risk factors for hepatocellular carcinoma include hepatitis B (HBV) or C virus (HCV) infection, smoking, alcohol, and aflatoxin [2]. Currently the prognosis for HCC is poor with Australian statistics indicating that the five year relative survival rate for primary liver cancers is only 16% [3]. The non-specific tyrosine kinase inhibitor sorafenib currently represents the only effective treatment against HCC [4]. This poor prognostic outlook and the limited availability of targeted molecular agents for HCC has led to the development of new therapies such as microRNAs (miRNAs).
miRNAs are short (19-24 nucleotides), non-coding RNA molecules that are post-transcriptional regulators of gene expression. Initially, miRNA is transcribed as primary miRNA (pri-miRNA), which is processed into precursor miRNA (pre-miRNA). This is then transported from the nucleus into the cytoplasm where it is processed into its mature form by the enzyme Dicer. The mature miRNA forms part of the RNA-induced silencing complex (RISC), which is responsible for regulating the output of protein-coding genes. These miRNAs interact with the 3’ untranslated regions (UTRs) of the protein-coding genes to result in a decrease in protein output via mRNA degradation or translational repression [5]. Alternatively, miRNAs can result in post-transcriptional stimulation of gene expression via a multitude of direct and indirect mechanisms [6]. It is estimated that a single miRNA can target hundreds to over one thousand different mRNAs, ultimately resulting in miRNAs being responsible for the regulation of around 20-30% of all protein-encoding genes [7]. These miRNAs have been reported to have key roles in cancer initiation, progression, and metastasis [8]. Oncogenic miRNAs are miRNAs that are up-regulated in cancer cells and promote carcinogenesis via the inhibition of tumour suppressor genes. Conversely, the miRNAs that are decreased in cancer cells are known as tumour suppressor miRNAs, as they normally inhibit proto-oncogenes to prevent cancer from developing [9]. The mammalian miRNA-34 family consists of miRNA-34a, which is encoded via its own individual transcript, and miRNA-34b and miRNA-34c, which possess a common primary transcript [10]. Due to the promising and extensive research conducted on miRNA-34a, this review article focused specifically on this particular isoform. Dysregulation of miRNA-34a has been implicated in a wide variety of cancers, including prostate, colon [11], and HCC [12]. The purpose of this review is to analyse the specific role of miRNA-34a in HCC, including addressing contradictory findings and investigating the recent clinical trials.
Table 1. Percentage of human HCC samples with decreased miRNA-34a expression compared to surrounding non-cancerous liver tissue.
The tumour suppressor role of miRNA-34a in hepatocellular carcinoma
A range of studies established that in the majority of human HCC samples, miRNA-34a expression was decreased in comparison to the surrounding non-cancerous liver tissue (Table 1) [12-16]. A murine model of hepatocarcinogenesis induced by a methyl-deficient diet also resulted in the down-regulation of miRNA-34a [17]. Low expression of miRNA-34a in HCC samples has been correlated with a shorter overall [13-15] and disease-free survival [14], as well as higher recurrence rates [13] when compared with samples that displayed up-regulation of miRNA-34a. The decreased expression of miRNA-34a is thought to be caused by genetic alterations such as deletions, point mutations, or chromosomal translocations of its genomic region 1p36 [18], which is common in HCC [19, 20]. Alternatively, this decreased expression has been linked to inactivating mutations of the p53 gene [18], as the induction of miRNA-34a is correlated with p53 status [21]. Furthermore, epigenetic silencing of miRNA-34a has been implicated with these decreased expression levels in multiple forms of cancer, via abnormal CpG methylation in its promoter region [22].
The administration of a miRNA-34a mimic (MRX34) has been shown to cause inhibition of a number of genes within multiple oncogenic pathways such as Wnt/ beta-catenin, c-MET, VEGF, hedgehog, and MAPK (all of which have been implicated in hepatocarcinogenesis), as well as stimulating multiple genes of the p53 pathway [23]. Daige et al. explored a diverse range of HCC related pathways, demonstrating how miRNA-34a exerts its anti-cancer effects by modulation of a number of genes responsible for processes such as metastasis, cellular proliferation, cell cycle regulation, apoptosis, and cellular senescence [23].
miRNA-34a and cellular proliferation, cell cycle regulation, and apoptosis
A number of cell culture studies investigated the effects of ectopic expression of miRNA-34a in the HepG2 cell line, with contradicting results [12,16,18]. Ectopic expression of miRNA-34a caused significant inhibition of cellular proliferation at 72 hours [18] and 96 hours [16] post- transfection. In addition, miRNA-34a was demonstrated to regulate the cell cycle via inducing G1 arrest [18]. Furthermore, it has been found that miRNA-34a can induce apoptosis, as determined by increased caspase 3/7 activity [16]. In contrast, other reports claimed that there was no effect on cellular proliferation, G1 arrest, or apoptosis, [12,18], highlighting the conflicting information within the current literature. The discrepancies between these three studies could partially be explained by the varying methods used to express miRNA-34a, and the different measurement times post-transfection (48, 72 or 96 hours) [16]. Additional research has found that miRNA-34a induces apoptosis in HCC cells via binding to the 3’ UTR of the Bcl-2 mRNA, causing inhibition of its translation [15]. Over-expression of miRNA-34a has also been correlated with a decreased expression of Bcl-2 in a number of other HCC studies [14,24].
miRNA-34a and metastasis
Down-regulation of miRNA-34a expression has been associated with metastatic HCC [12,16,25]. Multiple studies have established that the ectopic[1] expression of miRNA-34a in the HepG2 cell line inhibits tumour cell migration and invasion via silencing of the c-Met gene, which subsequently decreases the c-Met-induced phosphorylation of extracellular signal-regulated kinases 1 and 2 (ERK1/2) [12,16]. Cheng et al. also proposed that miRNA-34a prevents tumour migration, invasion, and metastasis by decreasing cathepsin D [18], a protease that contributes to the degradation of the basement membrane [26]. Furthermore in the HCC cell line Hca-F (high lymphatic metastatic potential) it was determined through in vitro and in vivo studies in mice that the ectopic expression of miRNA-34a caused a reduction in the metastatic potential [27].
miRNA-34a and cellular senescence
Earlier studies showed that miRNA-34a induced cellular senescence via cell cycle arrest in pathways that were telomere-independent [13, 28]. Recently, miRNA-34a over-expression has been shown to induce senescence in HCC cells in a telomere-dependent manner, regulated by p53. This cellular senescence occurs by the inhibition of FoxM1 and c-Myc, which causes the inactivation of telomerase activity, resulting in telomere shortening (Figure 1) [13].
Figure 1. Telomere dependent pathway of miRNA-34a induced cellular senescence (adapted from Xu et al. [13]). High levels of miRNA-34a, which is regulated by p53, results in the inhibition of FoxM1 and c-Myc, causing the inactivation of telomerase, leading to telomere shortening and subsequently cellular senescence.
miRNA-34a delivery methods
There is a vast array of delivery systems, both viral and non-viral, that are used to increase miRNA expression. Both mechanisms are associated with advantages and disadvantages [29]. Rubone and MRX34 are two prominent non-viral delivery methods that have been investigated in HCC studies [23,24]. Rubone is a small molecular modulator of miRNA-34a that was shown to induce miRNA-34a expression selectively in HCC cells (although only those with wild-type or mutant p53, not with p53 deletion), causing inhibition of tumour growth both in vitro and in vivo in the HepG2 xenograft mouse model. Xiao et al. also found that this miRNA-34a modulator displayed similar or even greater anti-HCC activity than sorafenib, the current treatment for advanced HCC [24]. MRX34 is a double-stranded miRNA-34a mimic that is delivered by liposomes [30]. The systemic delivery of this molecule resulted in tumour regression during in vivo studies in two different xenograft mouse models (Hep3B and HuH7) of liver cancer [23]. An oncolytic adenoviral vector that co-expressed miRNA-34a and IL-24 has also been studied in a HCC model. This was found to cause increased anti-tumour activity both in vitro and in vivo, predominantly via the downregulation of SIRT1 and Bcl-2 [14].
Clinical trials
Currently there is an ongoing phase I trial of MRX34 [31], which commenced in April 2013 and was originally indicated for patients with primary liver cancer or cancers with metastasis to the liver [32]. It was then gradually expanded to include patients with other advanced solid tumours (with or without liver metastasis) and haematological malignancies (lymphoma and multiple myeloma) [31]. There were 75 patients with advanced solid tumours enrolled in this study and 30 of these had HCC [33]. This trial’s data revealed that partial responses to the treatment, as per the RECIST guidelines (Table 2) [34], were observed in one patient with HCC, one with melanoma, [33] and one with advanced renal cell carcinoma [35]. Furthermore a number of patients in this trial were found to have attained a stable disease state [35]. This interim phase I data also determined that MRX34 has a manageable safety profile [33]. A recent press release from MIRNA therapeutics has indicated that phase II clinical trials will commence by the end of 2016 and will consist of two studies, one on renal cell carcinoma and the other on melanoma [35]. In terms of HCC-specific trials with MRX34, the future direction is currently unclear and with limited data available at the present time it is difficult to draw any definitive conclusions.
Table 2. Revised RECIST guidelines [34]
Combination therapy
Yang et al. demonstrated that ectopic expression of miRNA-34a resulted in the sensitisation of HCC cells to sorafenib-induced apoptosis and toxicity via inhibiting expression of Bcl-2 [15]. Additionally, the administration of miRNA-34a was found to sensitise HCC cells to chemotherapy (cisplatin) in vitro through the AXL pathway [36]. The combination of a miRNA-34a mimic and C-met inhibitor also resulted in a greater inhibition of cell growth and induction of apoptosis in vitro than either of these two therapies alone [16]. However, to establish more definitive results, further research is required in this field, particularly in regards to clinical trials.
The oncogenic role of miRNA-34a in hepatocellular carcinoma
Conversely, a number of other studies have shown increased expression of miRNA-34a in both murine and human HCC tissues [37-41], suggesting it may have an oncogenic role in addition to its tumour suppressor role. A recent article has investigated these claims and found that miRNA-34a displays oncogenic properties in liver tumours with beta-catenin activation [40]. Increased beta-catenin activation is most commonly caused by mutations in the CTNNB1 gene (the gene encoding beta-catenin), and this is estimated to occur in 20-40% of HCCs [42]. Gougelet and colleagues demonstrated using ApcKO mice (ApcKO causes activation of the Wnt/beta-catenin pathway [43]) that administration of a miRNA-34a inhibitor (LNA-34a) caused increased expression of hepatocyte nuclear factor 4a. This leads to increased apoptosis predominantly via caspase 2 activation and decreased cell proliferation through inhibition of cyclin D1 (Figure 2). This theory was then postulated to complement the data of the studies listed in Table 1, by accounting for those samples that showed up-regulation of miRNA-34a expression. The disparity in results between studies is thought to be due to the varying causes of HCC [40]. For example, the majority of HCC samples from the studies in the Table 1 were HBV+, and this was found to be associated with a lower frequency of CTNNB1 mutations [44]. Conversely HCC resulting from HCV infection has been shown to have a higher rate of CTNNB1 mutations [45]. However, these findings contradict the theory that miRNA-34a has a tumour suppressor function, and with relatively limited research on this oncogenic pathway, further investigation is required. Studies investigating the concept of miRNA-34a having a tumour suppressor or oncogenic function depending on the cause of the tumour would also be important, as well as an investigation of the clinical implications of this relationship.
Figure 2. Role of miRNA-34a inhibitor in counteracting the oncogenic action of miRNA-34a in HCC with beta-Catenin activation (Adapted from Gougelet et al. [40]). The miRNA-34a inhibitor LNA-34a causes a reduction in β-catenin induced miRNA-34a expression which leads to an increased expression of HNF-4α. Subsequently cyclin D1 levels are reduced, leading to decreased cell proliferation and increased caspase 2 levels, leading to increased apoptosis. The combined effects of these two actions then leads to the decreased progression of the hepatocellular carcinoma.
Limitations
A number of limitations were identified within this review, particularly relating to the conflicting information and the limited availability of clinical trial results. Contradictory information was noted on a number of occasions, especially with the use of a miRNA-34a inhibitor for HCC, making it difficult to evaluate a clear clinical benefit to this potential therapy. The data surrounding the clinical trial was also restricted as the trial is ongoing. Subsequently, all the data had to be sourced from press releases and abstracts from presentations at conferences, which were all funded by MIRNA therapeutics; thus a potential conflict of interest was noted.
Conclusion
Results have indicated that miRNA-34a has a tumour suppressor function in HCC and is responsible for the down-regulation of a number of genes involved in carcinogenesis. There is, however, contradicting information described in studies investigating these parameters, highlighting the complexity of this topic. Rubone and MRX34 are two prominent miRNA-34a delivery systems that were shown to exert anti-tumour activity in pre-clinical models. Additionally, MRX34 has been commenced in a clinical phase I trial that is still currently ongoing, with a partial response already observed in one patient. However, the future of HCC-specific MRX34 trials remains unclear as limited information is currently available. Based on the promising results of miRNA-34a as a combination therapy, this is an area that requires further investigation through clinical trials. Conversely, other sources have found that miRNA-34a plays an oncogenic role in HCC, particularly in those with beta-catenin activation. Subsequently, it was demonstrated that miRNA-34a inhibitors should be used in these instances. Further research is necessary in order to ascertain the clinical implications of using a miRNA-34a mimic or inhibitor depending on the beta-catenin mutation status of the patient.
Conflicts of interest
None declared.
References
Park J-W, Chen M, Colombo M, Roberts LR, Schwartz M, Chen P-J, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35(9):2155-66.
Chuang S-C, Vecchia CL, Boffetta P. Liver cancer: Descriptive epidemiology and risk factors other than HBV and HCV infection. Cancer Lett. 2009;286(1):9-14.
Australian Institute of Health and Welfare. Cancer in Australia: an overview 2014 [Internet]. Canberra: Australian Institute of Health and Welfare; 2014 [updated 2015 Apr 16; cited 2016 Apr 2]. 220p. Available from: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129550202
Yim HJ, Suh SJ, Um SH. Current management of hepatocellular carcinoma: an Eastern perspective. World J Gastroenterol. 2015;21(13):3826-42.
Ling H, Fabbri M, Calin GA. MicroRNAs and other non-coding RNAs as targets for anticancer drug development. Nat Rev Drug Discov. 2013;12(11):847-65.
Vasudevan S. Posttranscriptional upregulation by microRNAs. Wiley Interdiscip Rev RNA. 2012;3(3):311-30.
Felekkis K, Touvana E, Stefanou C, Deltas C. MicroRNAs: a newly described class of encoded molecules that play a role in health and disease. Hippokratia. 2010;14(4):236-40.
Lin S, Gregory RI. MicroRNA biogenesis pathways in cancer. Nat Rev Cancer. 2015;15(6):321-33.
Misso G, Di Martino MT, De Rosa G, Farooqi AA, Lombardi A, Campani V et al. Mir-34: a new weapon against cancer? Mol Ther Nucleic Acids. 2014;3(9):e195.
Hermeking H. The miR-34 family in cancer and apoptosis. Cell Death Differ. 2010;17(2):193-9.
Saito Y, Nakaoka T, Saito H. MicroRNA-34a as a therapeutic agent against human cancer. J Clin Med. 2015;4(11):1951-9.
Li N, Fu H, Tie Y, Hu Z, Kong W, Wu Y et al. miR-34a inhibits migration and invasion by down-regulation of c-Met expression in human hepatocellular carcinoma cells. Cancer Lett. 2009;275(1):44-53.
Xu X, Chen W, Miao R, Zhou Y, Wang Z, Zhang L et al. miR-34a induces cellular senescence via modulation of telomerase activity in human hepatocellular carcinoma by targeting FoxM1/c-Myc pathway. Oncotarget. 2015;6(6):3988-4004.
Lou W, Chen Q, Ma L, Liu J, Yang Z, Shen J et al. Oncolytic adenovirus co-expressing miRNA-34a and IL-24 induces superior antitumor activity in experimental tumor model. J Mol Med. 2013;91(6):715-25.
Yang F, Li QJ, Gong ZB, Zhou L, You N, Wang S et al. MicroRNA-34a targets Bcl-2 and sensitizes human hepatocellular carcinoma cells to sorafenib treatment. Technol Cancer Res Treat. 2014;13(1):77-86.
Dang Y, Luo D, Rong M, Chen G. Underexpression of miR-34a in hepatocellular carcinoma and its contribution towards enhancement of proliferating inhibitory effects of agents targeting c-MET. PLoS ONE. 2013;8(4):e61054.
Tryndyak VP, Ross SA, Beland FA, Pogribny IP. Down-regulation of the microRNAs miR-34a, miR-127, and miR-200b in rat liver during hepatocarcinogenesis induced by a methyl-deficient diet. Mol Carcinog. 2009;48(6):479-87.
Cheng J, Zhou L, Xie QF, Xie HY, Wei XY, Gao F et al. The impact of miR-34a on protein output in hepatocellular carcinoma HepG2 cells. Proteomics. 2010;10(8):1557-72.
Herath NI, Kew MC, Whitehall VL, Walsh MD, Jass JR, Khanna KK et al. p73 is up-regulated in a subset of hepatocellular carcinomas. Hepatology. 2000;31(3):601-5.
Midorikawa Y, Yamamoto S, Tsuji S, Kamimura N, Ishikawa S, Igarashi H et al. Allelic imbalances and homozygous deletion on 8p23.2 for stepwise progression of hepatocarcinogenesis. Hepatology. 2009;49(2):513-22.
Bommer GT, Gerin I, Feng Y, Kaczorowski AJ, Kuick R, Love RE et al. p53-mediated activation of miRNA34 candidate tumor-suppressor genes. Curr Biol. 2007;17(15):1298-307.
Lodygin D, Tarasov V, Epanchintsev A, Berking C, Knyazeva T, Korner H et al. Inactivation of miR-34a by aberrant CpG methylation in multiple types of cancer. Cell Cycle. 2008;7(16):2591-600.
Daige CL, Wiggins JF, Priddy L, Nelligan-Davis T, Zhao J, Brown D. Systemic delivery of a miR34a mimic as a potential therapeutic for liver cancer. Mol Cancer Ther. 2014;13(10):2352-60.
Xiao Z, Li CH, Chan SL, Xu F, Feng L, Wang Y et al. A small-molecule modulator of the tumor-suppressor miR34a inhibits the growth of hepatocellular carcinoma. Cancer Res. 2014;74(21):6236-47.
Budhu A, Jia HL, Forgues M, Liu CG, Goldstein D, Lam A et al. Identification of metastasis-related microRNAs in hepatocellular carcinoma. Hepatology. 2008;47(3):897-907.
Khalkhali-Ellis Z, Hendrix MJC. Elucidating the function of secreted maspin: inhibiting cathepsin D–mediated matrix degradation. Cancer Res. 2007;67(8):3535-9.
Guo Y, Li S, Qu J, Wang S, Dang Y, Fan J et al. MiR-34a inhibits lymphatic metastasis potential of mouse hepatoma cells. Mol Cell Biochem. 2011;354(1-2):275-82.
Chen F, Hu SJ. Effect of microRNA-34a in cell cycle, differentiation, and apoptosis: a review. J Biochem Mol Toxicol. 2012;26(2):79-86.
Zhang Y, Wang Z, Gemeinhart RA. Progress in microRNA delivery. J Control Release. 2013;172(3):962-74.
Agostini M, Knight RA. miR-34: from bench to bedside. Oncotarget. 2014;5(4):872-81.
Mirna Therapeutics Inc; Cancer Prevention Research Institute of Texas. A multicenter phase I study of MRX34, microRNA miR-RX34 liposomal injection. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2013 [cited 2016 Apr 3]. Available from: https://clinicaltrials.gov/ct2/show/study/NCT01829971?view=results. NLM Identifier: NCT01829971
Bouchie A. First microRNA mimic enters clinic. Nat Biotech. 2013;31(7):577.
Beg MS, Brenner A, Sachdev J, Ejadi S, Borad M, Kang Y-K et al. Safety, tolerability, and clinical activity of MRX34, the first-in-class liposomal miR-34 mimic, in patients with advanced solid tumors [Abstract]. Mol Cancer Ther. 2015;14(12 S2):C43.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-47.
MIRNA Therapeutics. Mirna therapeutics provides operational update & reports financial results for fourth quarter and full year ended December 31, 2015 [Internet]. Austin Texas: MIRNA Therapeutics; 2016 Mar 29 [cited 2016 Apr 3]. Available from: http://investor.mirnarx.com/releasedetail.cfm?ReleaseID=962545.
Li X-Y, Wen J-Y, Jia C-C, Wang T-T, Li X, Dong MIN et al. MicroRNA-34a-5p enhances sensitivity to chemotherapy by targeting AXL in hepatocellular carcinoma MHCC-97L cells. Oncol Lett. 2015;10(5):2691-8.
Pineau P, Volinia S, McJunkin K, Marchio A, Battiston C, Terris B et al. miR-221 overexpression contributes to liver tumorigenesis. Proc Natl Acad Sci USA. 2010;107(1):264-9.
Sukata T, Sumida K, Kushida M, Ogata K, Miyata K, Yabushita S et al. Circulating microRNAs, possible indicators of progress of rat hepatocarcinogenesis from early stages. Toxicol Lett. 2011;200(1-2):46-52.
Zhu L, Gao J, Huang K, Luo Y, Zhang B, Xu W. miR-34a screened by miRNA profiling negatively regulates Wnt/β-catenin signaling pathway in Aflatoxin B1 induced hepatotoxicity. Sci Rep. 2015;5:16732.
Gougelet A, Sartor C, Bachelot L, Godard C, Marchiol C, Renault G et al. Antitumour activity of an inhibitor of miR-34a in liver cancer with beta-catenin-mutations. Gut [Internet]. 2015 Mar 19. Available from: http://gut.bmj.com/content/65/6/1024.long [Epub ahead of print].
Pok S, Wen V, Shackel N, Alsop A, Pyakurel P, Fahrer A et al. Cyclin E facilitates dysplastic hepatocytes to bypass G1/S checkpoint in hepatocarcinogenesis. J Gastroenterol Hepatol. 2013;28(9):1545-54.
Tornesello ML, Buonaguro L, Tatangelo F, Botti G, Izzo F, Buonaguro FM. Mutations in TP53, CTNNB1 and PIK3CA genes in hepatocellular carcinoma associated with hepatitis B and hepatitis C virus infections. Genomics. 2013;102(2):74-83.
Colnot S, Decaens T, Niwa-Kawakita M, Godard C, Hamard G, Kahn A et al. Liver-targeted disruption of Apc in mice activates beta-catenin signaling and leads to hepatocellular carcinomas. Proc Natl Acad Sci USA. 2004;101(49):17216-21.
Guichard C, Amaddeo G, Imbeaud S, Ladeiro Y, Pelletier L, Maad IB et al. Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma. Nat Genet. 2012;44(6):694-8.
Li M, Zhao H, Zhang X, Wood LD, Anders RA, Choti MA et al. Inactivating mutations of the chromatin remodeling gene ARID2 in hepatocellular carcinoma. Nat Genet. 2011;43(9):828-9.
Chronic myeloid leukaemia (CML) is a myeloproliferative disorder caused by BCR-ABL1 igureusion encoding for a tyrosine kinase oncoprotein. Since the introduction of the tyrosine kinase inhibitor (TKI), imatinib, in 2000, CML survival rates have increased, to the point where life expectancy is equal to that of the general population. One obstacle patients face is imatinib resistance. Literature about resistance has mainly focussed on mutations in the Bcr-Abl kinase domain (KD), which have been well described. Areas that have not been as well established include the origin of KD mutations and resistance from mechanisms outside of KD mutations. This review focuses on how KD mutations arise and their mechanisms of resistance and the roles of BCR-ABL1 gene amplification, Erk1, and Lyn kinase in creating resistance outside of the KD. Experimental therapies to combat imatinib resistance are also mentioned. Using database searches to obtain the current literature, this review attempts to determine the current consensus on these topics and highlight areas where research could be beneficial. While the origin of KD-mutations and non-KD resistance is not entirely clear, the many possible causes that have been elucidated thus far have already paved the way for new therapies.
Introduction
Chronic myeloid leukaemia (CML) was the first cancer where the pathological chromosomal abnormality was identified, and is one of the most understood and well-managed cancers [1,2]. CML is a clonal disorder of pluripotent stem cells that results in over-proliferation of mature myeloid cells [3]. Constitutive and aberrant tyrosine kinase activity is responsible for pathological cell proliferation in CML [4].
Before the advent of tyrosine kinase inhibitors (TKIs), 5-year survival rate for patients aged 20-44 was 40%, and less than 20% for patients over 65 years. For patients aged 15-44 diagnosed in 2000, this jumped to 71.6%, increasing to 86.4%, if diagnosed in 2005 [5]. Responsible for these leaps in survival was imatinib mesylate, a TKI approved in 2001 [6]. Imatinib antagonises tyrosine kinase activity by competing with ATP binding to the Bcr-Abl protein, reducing unchecked cell-cycle progression [3]. Imatinib resistance undermines therapy, putting patients at risk, and occurs in approximately 25% of patients [1]. Hence, it is important for doctors and medical students alike to understand that resistance occurs, some of the mechanisms behind resistance and how new pharmacotherapies can combat these. This review summarises the pathophysiology of CML and synthesises the literature around competing theories of imatinib resistance.
Pathophysiology of CML
CML is a myeloproliferative disease caused by a reciprocal translocation between chromosome 9 and 22 (9;22)(q34;q11.2)[1,7]. This creates an abnormal chromosome 22 called the Philadelphia (Ph) chromosome, named after the city it was discovered in in 1960 [2,8]. The oncogenic effects of this translocation are caused by 5’ exons of the BCR (breakpoint cluster region) gene fusing to the 3’ exons of ABL1 (Abelson tyrosine protein kinase 1) [3]. This creates the BCR-ABL1 oncogene on the Ph chromosome encoding for Bcr-Abl tyrosine kinase, or p210BCR/ABL [9-11]. Retroviral insertion of p210BCR-ABL in murine models induces a myeloproliferative disorder similar to CML [11]. However, in less than 10% of cases, gene fusion occurs in different exons creating kinases p190 or p230 depending on where the fusion occurs [12,13]. Bcr-Abl has constitutive tyrosine kinase activity, causing modulated gene transcription, proliferation, and enforced survival of myeloid progenitor cells [14]. Unregulated cells grow and enter the S-Phase of the cell cycle independently of physiological growth factors and avoid apoptosis [8,14,15]. Abl and Bcr-Abl are non-receptor tyrosine kinases that travel between the nucleus and the cytoplasm and phosphorylate proteins via SH2 and SH3 domains [16].
Figure 1. Intracellular pathways influenced by Bcr-Abl Kinase [24,25,26]. A synthesis and simplification of selected pathways (JAK/STAT, Gab2, Lyn kinase, IGF-1 and β-1 integrin) showing the leukaemogenic downstream effects of Bcr-Abl signalling. Imatinib is shown solely inhibiting Bcr-Abl, however, research shows imatinib therapy also affects Lyn kinase expression and activity.Targets of increased phosphorylation that have proliferative effects include insulin-like growth factor receptor 1 (IGF-1R) [17], Ras [16], p27Kip [18], and others. This review will focus on a selection of the most well-known pathways (Figure 1). Bcr-Abl regulates IGF-1R expression via Stat5, which enhances IGF-1R gene expression [19,20]. IGF-1R tyrosine kinase stimulates haematopoietic stem cells and CML patients show higher than normal levels of IGF-1R mRNA [17]. When CML cells were treated with an inhibitor of tyrosine kinase phosphorylation of IGF-1R, the cells underwent apoptosis, cell-cycle arrest, and decreased cell proliferation, illustrating how IGF-1R and CML are linked [17]. One protein both IGF-1R and Bcr-Abl stimulate is Ras [21]. Ras is a well-studied oncoprotein that regulates several downstream pathways that increase cell proliferation including PI3/AKT and JAK/STAT [16]. The importance of Ras in CML pathophysiology was confirmed when association of Bcr-Abl and Ras was blocked and subsequent attempts to induce a CML-like disorder failed [22]. P27Kip is a cyclin dependent kinase (cdk) inhibitor and decreases cdk2 activity, thus inhibiting G1/S-phase progression. In CML, while the amount of P27Kip is unchanged, 80% of P27Kip is relocated to the cytoplasm, where it cannot interact with nucleic cdk2, allowing unregulated cell-cycle progression [18]. This is caused by Bcr-Abl interfering with cytoskeletal proteins such as 1-integrins [23]. These three pathways highlight that Bcr-Abl is central to CML pathology[11]. As a consequence, pharmacotherapy targeting Bcr-Abl has been developed in the form of imatinib.
Imatinib
Imatinib is a TKI hailed as a conceptual breakthrough in targeted chemotherapy, and is the first line treatment in CML, while also being used in Ph+ acute lymphocytic leukaemia and some gastric cancers [27]. In early evaluation studies, it was found to specifically inhibit cellular proliferation and tumour formation of Bcr-Abl expressing cells by 92%-98% [28]. Imatinib is effective when compared to other early treatments for CML, increasing the likelihood of survival at ten years by 20% when compared to the closest alternative therapy (Figure 2) [29]. The current parameters to measure successful treatment outcomes are listed with definitions in Table 1. In the International Randomized Study of Interferon and STI571, it was found that complete haematological response (CHR), complete cytogenetic response (CCyR), and major molecular response (MMR) scores were superior in imatinib-treated patients compared with interferon-treated patients [30]. Additionally, in the original trials for imatinib approval, three phase II studies involving 1027 patients showed over 90% of patient leukocyte counts returned to normal, and when combined with interferon, 100% of evaluable patients achieved CHR [31].
Figure 2. Survival with CML over time [29]. This figure from the German CML-Study group shows patient survival probability as a function of time after diagnosis in five consecutive randomised treatment optimisation studies.
Table 1. Measurements of CML therapy outcome [1,32]
Mechanism of action
Bcr-Abl has an activation loop, a P-loop with an ATP binding site (in the kinase domain) and substrate anchoring SH2 and SH3 domains [33,34,35]. Imatinib binds specifically to the ATP-binding sites of Bcr-Abl, c-kit, and platelet-derived growth factor receptors, and inhibits their tyrosine kinase activity by both preventing ATP binding and stabilising the activation loop in an inactive conformation [34,36,37]. When Bcr-Abl tyrosine kinase activity is inhibited, there is no downstream signalling and treatment is successful in 77% of all patients [1] and virtually 100% of patients treated in the early stages of the disease [34]. The European LeukemiaNet (ELN) 2013 guidelines use MMR as the marker to indicate success of TKI therapy [32], however, Thompson et al. [1]. have argued that MMR overestimates the number of patients with treatment failure.
Treatment considerations and mechanisms of Imatinib resistance in CML
Failure of TKI therapy is caused by a number of factors, including inappropriate drug choice, patient non-adherence, and drug resistance. There are a number of opinions as to what constitutes treatment failure, but the definition used by this paper is the one put forward by the ELN and European Society for Medical Oncology. Treatment failure depends on which measurement is used; using haematological parameters (testing peripheral leukocyte counts), treatment failure is defined as no haematological response by three months, or any loss of CHR. Using cytogenetic response, however, treatment failure is no cytogenetic response within six months, no CCyr by 18 months, or any loss of CCyr, as detected by CBA [38]. Finally, a sub-optimal molecular response is defined as no MMR by 18 months or loss of MMR at any point using PCR for BCR-ABL1 transcripts [38]. While this review focuses on imatinib (the gold standard in CML therapy) [30], second generation TKIs such as nilotinib, ponatinib, and dasatinib are now also used, both as first line agents and for use in imatinib resistant patients [1,27]. Which TKI to use and at what dose depends on a number of factors, including imatinib sensitivity and which disease phase the patient is in. CML is staged into chronic phase (CP), accelerated phase (AP), and blast phase (BP) (Table 2) [39]. For instance, a patient in AP who has never had a TKI is still treated with imatinib, but if they have taken imatinib and then progressed to AP, a second generation TKI is used [1]. Using imatinib inappropriately could cause treatment failure, while immediately using a second generation TKI or increasing TKI dosages has been found to limit adherence, as well as side effects (Table 2), especially for patients who require more potent TKIs and higher doses [40].
Table 2. Stages of CML with respective treatment options and side effects[1,27,41,42].The most serious complication in CML treatment is resistance to therapy. This occurs most frequently in the AP and BP stages of the disease22. Traditionally, resistance is thought to occur from point mutations in the Bcr-Abl kinase domain (KD) [1,15,34,43]. There are several mutations that can cause mutations in this setting (Table 3). Bcr-Abl KD mutations can be intrinsic (primary) or acquired (secondary) and interfere with TKI therapy in a number of ways [1]. The most common mechanisms are by directly interfering with TKI binding via amino acid substitutes in the ATP binding site or by preventing the activation loop from adopting the inactive conformational state [34]. Although Abl KD mutations causing TKI resistance were first induced in laboratory cell lines in 2000 [44], and detected in vivo clinically in 2001 [45], novel mutations are continually being discovered, with two new mutations conferring resistance sequenced in 2014 [46]. The discovery and sequencing of mutations has led to individualised therapy and a more accurate prognosis for specific mutations, for instance the T315I mutation. In this common mutation, threonine-315 is replaced with isoleucine, effectively removing a hydrogen-bonding site required for TKI binding resulting in enormous treatment difficulty [34]. Only one TKI has any activity in T315I+ patients and that is the highly potent ponatinib. However, this drug is not used as a front line therapy as it has a higher rate of arterial thrombosis and pancreatitis when compared to imatanimb [1]. A novel drug that binds to a nearby site not affected by the mutation, HS-438, is being investigated for use in T315I+ CML and has shown success in pre-clinical trials [47]. Another drug, ABL001, also acts at another molecular site and thus avoids the resistance caused by KD mutations. ABL001 mimics the autoregulating region of ABL1 that is lost upon fusion of BCR, restoring negative regulation, and has been shown to remain effective against clinically significant mutations in an in vivo model [48]. This example highlights how sequencing mutations can provide valuable, individualised prognostic information and guide future research.
Table 3. Sample of p210BCR/ABL kinase domain mutations known to cause resistance [1,34,49-51]. *Incidence based off Ursan et al.’s meta-analysis of a total of 1,698 patients. Overall mutation rate for imatinib was 9.7% [50].How these mutations arise is not clear; in some patients with secondary resistance pre-therapeutic samples revealed the same KD mutation detected at relapse, consistent with selection of pre-existing resistant clones during therapy giving an evolutionary advantage [52,53]. There is some contention as to whether these stem cell mutations can cause primary resistance or whether KD point mutations can only cause secondary resistance and relapse. Previous studies have concluded that Bcr-Abl KD mutations are a rare cause for primary resistance, however, more recent research found KD mutations in 56% of patients with primary resistance [54,55]. This discrepancy may be explained by the more recent study utilising more sensitive technology and patients who had CML for a longer period of time, which has been linked to mutagenicity [28]. KD resistance in Bcr-Abl1 CML differs from other diseases in that unlike traditional drug resistance, where treatment resistance arises via positive selection of tumour cells with mechanisms to avoid DNA damage, in CML resistant cells there is a tendency to accumulate more rather than less DNA damage [56]. The mechanism behind this is unknown, but it is an example of how the malignancy directly causes resistance. Nevertheless, the evidence suggests that pre-existing KD mutations in cancer stem cells are more likely to be responsible for secondary resistance.
Other research suggests that BCR-ABL1 has the ability to cause self-mutagenesis. Mutation rate and advanced disease phase were correlated, consistent with mutations being related to exposure time to Bcr-Abl activity [34]. One suggested mechanism is production of reactive oxygen species causing genomic instability, shown in vitro and in murine models, but beyond the original studies, no further research has been undertaken [34,57]. While KD mutations are a highly researched area in CML therapy (over 60 unique point mutations have been identified), there remains an information deficit, for example, the prevalence of mutations in specific populations, or randomised controlled trials for TKI choice following imatinib failure [1,58].
Non Bcr-Abl kinase domain mediated resistance
Recent research adds complexity by suggesting there are a number of mutations and events occurring outside of Bcr-Abl KD that impact drug resistance [43].This includes mutations of Bcr-Abl1 outside of the kinase domain, such as BCR-ABL1 amplification, and causes outside of the Bcr-Abl1 protein altogether, such as mesenchymal cells, drug transporters and bypass molecular pathways. Increased BCR-ABL1 expression via gene amplification is found in most TKI resistant cells, whether the mutations are primary, secondary, KD, or non-KD, implying a link between increased expression and resistance [59]. However, increased expression is not the sole cause of non-KD mediated resistance as studies have shown that increasing imatinib concentration in non-mutated, sensitive cells with induced BCR-ABL1 amplification still reduces Bcr-Abl activity, whereas some resistant cells without KD mutations remain resistant at any dose [60].
Extracellular Signal-Regulated Kinase 2 (Erk2) is a Mitogen Activated Protein Kinase (MAPK) and has been implicated in both primary and secondary resistance (i.e. immediate resistance to therapy and resistance that builds over time)[60,61]. In a study of non-KD mutated resistant cells treated with imatinib, Erk2 was found in the nucleus of resistant cells only, and inhibiting Erk2 caused damage to resistant cells [60]. Mechanisms for how Erk2 could cause primary resistance were then elucidated. To achieve this, mutated Ras (which activates Erk2), was virally transduced into sensitive cells that were cultured and treated with imatinib. Using proliferation assays to determine cell survival, it was discovered activating Erk2 gave previously sensitive cells resistance without any prior exposure to imatinib. Erk2 is a key regulator of the pro-apoptotic molecule Bim and it is proposed interactions between Erk2 and Bcr-Abl over-stimulate Erk2 and reduce CML cell apoptosis [62]. Research in 2016 by Wong et al. [63] extended these results to create a pharmacotherapy inhibiting Erk2, showing areas outside of the KD can cause primary and secondary resistance and can be targeted.
Lyn kinase
Lyn kinase is a non-receptor tyrosine kinase regulated by Bcr-Abl. Imatinib resistant but Bcr-Abl KD-mutation negative cells were found to overexpress Lyn kinase following treatment with imatinib [64]. In cell lines from these patients, while imatinib effectively inhibited Bcr-Abl activity, Lyn kinase phosphorylation continued, allowing proliferation to continue. Interestingly, prior to imatinib therapy, there was no consistent difference in Lyn expression between sensitive and resistant cells, but afterward there were consistent distinctions in their control of phosphorylation. This implies imatinib treatment uncouples Lyn expression from Bcr-Abl, leading to resistance. Lyn overexpression can induce a three to fourfold resistance, equal to some KD mutations, yet the mechanisms of its overexpression and how it worsens CML are not yet known [65]. One theory is that because silencing of Lyn kinase induces apoptosis in CML cells, overexpression causes cell survival, signalled through via Gab2 [66,67]. The fact that this effect is not seen in imatinib-naïve CML patient cells supports the idea that Lyn kinase only causes acquired resistance, leaving the mechanisms behind primary resistance a mystery.
Drug transporters
Alterations in drug transporters are yet another mechanism by which medication resistance can occur and will be mentioned briefly. A drug must both reach the target organ in sufficient amounts and be present at an effective therapeutic concentration for it to exert and effect, and both influx and efflux transporters can interfere with these pharmacokinetics [27]. Radiolabelled imatinib assays have determined that the level of kinase inhibition is dependent on the level of uptake and retention of imatinib achieved [68]. Imatinib enters the circulation from the gastrointestinal tract by a member of the organic cation transporter (OCT) family, OCT-1, thus mutations in OCT-1 are thought to contribute to treatment failure [68]. Conversely, imatinib leaves the cell via the p-glycoprotein multidrug resistance protein-1 (MDR1 or ABCB1) [69]. In other drugs, MDR1 overexpression has been confirmed to cause drug resistance by increasing efflux before a therapeutic concentration can be reached, and this is a relationship currently under investigation in CML.
Non-Bcr-Abl KD resistance is not a well-studied area and much research is yet to be undertaken. Two recent CML mutation reviews by Jabbour et al. and O’Hare et al. only provide a brief mention of non Bcr-Abl mutations causing resistance, even though these mutations cause from 10%-40% of TKI resistance [3,70]. In addition, there was much disagreement among researchers concerning molecular pathways to resistance. Erk2 is part of a super-family of MAPKs, other members such as Erk1, Erk5, and P38MAPK, have been considered in imatinib resistance [71,72]. Aceves-Luquero et al. carried out knock-out studies of MAPKs, which identified only Erk2 as having a resistance-inducing effect [52]. Extremely resistant patients require potent TKIs or stem-cell transplantation, both of which greatly affect quality of life, which could be avoided if mechanisms behind resistance were uncovered and targeted treatment developed1.
Limitations
While p210BCR-ABL accounts for 90% of cases of CML, other Bcr-Abl variants were not examined despite their different treatment responses, limiting the applicability of this review. Furthermore, the diagram in Figure 1 is a simplified representation of the pathways associated with Bcr-Abl, especially in the case of JAK/STAT. Only pathways that have been clearly implicated in CML and imatinib resistance by research literature were included. Systematic database searches were used to carry out this review. Spelling and terminology variations that influence search results, for example, “myeloid” and “myelogenous”, were a limiting factor.
Clinical implications
This article holds a number of clinical implications for all medical students, not just the aspiring oncologist. For instance, the prevailing view in oncology is that mutations that confer imatinib resistance occur in the kinase domain. With the explosion of advances in genome sequencing, it is becoming possible to prospectively genetically screen patients to determine whether resistance will occur. If the current wisdom regarding CML resistance prevails, then mutations outside the kinase domain (that have been reported to cause between 10% – 40% of resistance) could be ignored, potentially putting patients at risk of ineffective treatment which could cost them their lives [2]. By investigating and becoming aware of the role of non-KD mutations, doctors could also give more accurate prognoses to patients with these mutations and begin studies looking at the best treatment for these cases (for example, randomised controlled trials comparing current therapy to higher doses of imatinib, or new pharmacological agents altogether). This review also provides a general overview into CML pathophysiology, imatinib pharmacology and chemotherapy resistance, topics every medical practitioner should be very familiar with.
Conclusion
Imatinib is a TKI that revolutionised leukaemia treatment and increased the length and quality of life of CML patients. While it has been known for many years that primary and secondary resistance to imatinib exist, the mechanisms have not been fully explained. While mutations in the Bcr-Abl KD account for the majority of resistance and are well known, what remains unclear is the origin of these mutations, and how resistance occurs without KD mutations. Stem cell mutations and self-mutagenesis are possible explanations for how KD mutation occurs, and gene amplification, Lyn kinase and Erk2 for resistance occurring outside of the KD. Further research identifying key events in downstream pathways will offer new approaches for overcoming all forms of imatinib resistance.
Acknowledgements
The author would like to thank and acknowledge A/Prof Peter Johnson and A/Prof Bill Warren of James Cook University School of Medicine and Dentistry who provided comments and feedback on this paper. The author would also like to thank Dr. Donna Rigano and Miss Shalisa Maisrikrod for their assistance and editing help.
Conflicts of interest
None declared
References
Thompson PA, Kantarjian HM, Cortes JE. Diagnosis and treatment of chronic myeloid leukemia in 2015. Mayo Clinic proceedings. 2015;90(10):1440-54.
Nowell P HD. A minute chromosome in human chronic granulocytic leukemia. Science. 1960;132:1497.
Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2014 update on diagnosis, monitoring, and management. Am J Haematol. 2014;89(5):547-56.
An X, Tiwari AK, Sun Y, Ding PR, Ashby CR, Jr., Chen ZS. BCR-ABL tyrosine kinase inhibitors in the treatment of Philadelphia chromosome positive chronic myeloid leukemia: a review. Leukemia research. 2010;34(10):1255-68.
Brunner AM, Campigotto F, Sadrzadeh H, Drapkin BJ, Chen YB, Neuberg DS, et al. Trends in all-cause mortality among patients with chronic myeloid leukemia: a surveillance, epidemiology, and end results database analysis. Cancer. 2013;119(14):2620-9.
Cohen MH, Williams G, Johnson JR, Duan J, Gobburu J, Rahman A, et al. Approval summary for imatinib mesylate capsules in the treatment of chronic myelogenous leukemia. Clinical cancer research : an official journal of the American Association for Cancer Research. 2002;8(5):935-42.
JD R. A new consistent chromosomal abnormality in chromc myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature. 1973;243:290-3.
Holtz MS, Forman SJ, Bhatia R. Nonproliferating CML CD34+ progenitors are resistant to apoptosis induced by a wide range of proapoptotic stimuli. Leukemia. 2005;19(6):1034-41.
Rafiei A, Mian AA, Doring C, Metodieva A, Oancea C, Thalheimer FB, et al. The functional interplay between the t(9;22)-associated fusion proteins BCR/ABL and ABL/BCR in Philadelphia chromosome-positive acute lymphatic leukemia. PLoS genetics. 2015;11(4):e1005144.
McLaughlin J, Chianese E, Witte ON. In vitro transformation of immature hematopoietic cells by the P210 BCR/ABL oncogene product of the Philadelphia chromosome. Proceedings of the National Academy of Sciences of the United States of America. 1987;84(18):6558-62.
Daley GQ, Van Etten RA, Baltimore D. Induction of Chronic Myelogenous Leukemia in Mice by the P210$^{bcr/abl}$ Gene of the Philadelphia Chromosome. Science. 1990;247(4944):824-30.
Arana-Trejo RM, Ruiz Sanchez E, Ignacio-Ibarra G, Baez de la Fuente E, Garces O, Gomez Morales E, et al. BCR/ABL p210, p190 and p230 fusion genes in 250 Mexican patients with chronic myeloid leukaemia (CML). Clinical and laboratory haematology. 2002;24(3):145-50.
Chan LC, Karhi KK, Rayter SI, Heisterkamp N, Eridani S, Powles R, et al. A novel abl protein expressed in Philadelphia chromosome positive acute lymphoblastic leukaemia. Nature. 1987;325(6105):635.
Hershkovitz-Rokah O, Modai S, Pasmanik-Chor M, Toren A, Shomron N, Raanani P, et al. Restoration of miR-424 suppresses BCR-ABL activity and sensitizes CML cells to imatinib treatment. Cancer letters. 2015;360(2):245-56.
Jonuleit T, Peschel C, Schwab R, van der Kuip H, Buchdunger E, Fischer T, et al. Bcr-Abl kinase promotes cell cycle entry of primary myeloid CML cells in the absence of growth factors. British journal of haematology. 1998;100(2):295-303.
Bertacchini J, Ketabchi N, Mediani L, Capitani S, Marmiroli S, Saki N. Inhibition of Ras-mediated signaling pathways in CML stem cells. Cell Oncol. 2015;38(6):407-18.
Shi P, Chandra J, Sun X, Gergely M, Cortes JE, Garcia-Manero G, et al. Inhibition of IGF-IR tyrosine kinase induces apoptosis and cell cycle arrest in imatinib-resistant chronic myeloid leukaemia cells. Journal of cellular and molecular medicine. 2010;14(6B):1777-92.
Jiang Y, Zhao RC, Verfaillie CM. Abnormal integrin-mediated regulation of chronic myelogenous leukemia CD34+ cell proliferation: BCR/ABL up-regulates the cyclin-dependent kinase inhibitor, p27Kip, which is relocated to the cell cytoplasm and incapable of regulating cdk2 activity. Proceedings of the National Academy of Sciences of the United States of America. 2000;97(19):10538-43.
Lakshmikuttyamma A, Pastural E, Takahashi N, Sawada K, Sheridan DP, DeCoteau JF, et al. Bcr-Abl induces autocrine IGF-1 signaling. Oncogene. 2008;27(27):3831-44.
Xie J, Chen X, Zheng J, Li C, Stacy S, Holzenberger M, et al. IGF-IR determines the fates of BCR/ABL leukemia. Journal of hematology & oncology. 2015;8:3.
Zha J, Lackner MR. Targeting the insulin-like growth factor receptor-1R pathway for cancer therapy. Clinical cancer research : an official journal of the American Association for Cancer Research. 2010;16(9):2512-7.
Million RP, Van Etten RA. The Grb2 binding site is required for the induction of chronic myeloid leukemia-like disease in mice by the Bcr/Abl tyrosine kinase. Blood. 2000;96(2):664-70.
Bhatia R, Verfaillie CM. Inhibition of BCR-ABL expression with antisense oligodeoxynucleotides restores beta1 integrin-mediated adhesion and proliferation inhibition in chronic myelogenous leukemia hematopoietic progenitors. Blood. 1998;91(9):3414-22.
Sattler M, Mohi MG, Pride YB, Quinnan LR, Malouf NA, Podar K, et al. Critical role for Gab2 in transformation by BCR/ABL. Cancer Cell. 2002;1(5):479-92.
Goss VL, Lee KA, Moritz A, Nardone J, Spek EJ, MacNeill J, et al. A common phosphotyrosine signature for the Bcr-Abl kinase. Blood. 2006;107(12):4888-97.
O’Hare T, Deininger MW, Eide CA, Clackson T, Druker BJ. Targeting the BCR-ABL signaling pathway in therapy-resistant Philadelphia chromosome-positive leukemia. Clin Cancer Res. 2011;17(2):212-21.
Rang HP RJ, Flower RJ, Henderson G. Anti-Cancer Drugs. Rang & Dale’s Pharmacology. 8th Edition ed. Philadelphia, Pennsylvania: Elsevier; 2015. p. 687-8.
Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, et al. Effects of a selective inhibitor of the Abl tyrosine kinase on the growth of Bcr-Abl positive cells. Nature medicine. 1996;2(5):561-6.
Hehlmann R. CML—where do we stand in 2015? Annals of Hematology. 2015;94(2):103-5.
O’Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. The New England journal of medicine. 2003;348(11):994-1004.
Habeck M. FDA licences imatinib mesylate for CML. The Lancet Oncology. 2002;3(1):6.
Baccarani M, Deininger MW, Rosti G, Hochhaus A, Soverini S, Apperley JF, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013;122(6):872-84.
Segaliny AI, Tellez-Gabriel M, Heymann MF, Heymann D. Receptor tyrosine kinases: Characterisation, mechanism of action and therapeutic interests for bone cancers. Journal of bone oncology. 2015;4(1):1-12.
O’Hare T, Eide CA, Deininger MW. Bcr-Abl kinase domain mutations, drug resistance, and the road to a cure for chronic myeloid leukemia. Blood. 2007;110(7):2242-9.
Ren SY, Xue F, Feng J, Skorski T. Intrinsic regulation of the interactions between the SH3 domain of p85 subunit of phosphatidylinositol-3 kinase and the protein network of BCR/ABL oncogenic tyrosine kinase. Experimental hematology. 2005;33(10):1222-8.
Buchdunger E, Zimmermann J, Mett H, Meyer T, Muller M, Druker BJ, et al. Inhibition of the Abl protein-tyrosine kinase in vitro and in vivo by a 2-phenylaminopyrimidine derivative. Cancer research. 1996;56(1):100-4.
Kantarjian HM, Cortes JE, O’Brien S, Giles F, Garcia-Manero G, Faderl S, et al. Imatinib mesylate therapy in newly diagnosed patients with Philadelphia chromosome-positive chronic myelogenous leukemia: high incidence of early complete and major cytogenetic responses. Blood. 2003;101(1):97-100.
Jabbour E, Cortes JE, Kantarjian HM. Suboptimal response to or failure of Imatinib treatment for chronic myeloid leukemia: what is the optimal strategy? Mayo Clinic proceedings. 2009;84(2):161-9.
World Health Organization Classification of Tumors of Haematopoietics and Lymphoid Tissues. . In: Swerdlow SH CE, Harris NL, et al, editor. Lyon, France: IARC Press; 2008.
Branford S, Yeung DT, Prime JA, Choi SY, Bang JH, Park JE, et al. BCR-ABL1 doubling times more reliably assess the dynamics of CML relapse compared with the BCR-ABL1 fold rise: implications for monitoring and management. Blood. 2012;119(18):4264-71.
Australian public assessment report for Imatinib, Nilotinib and Dastinib. In: Administration TG, editor. Woden, ACT, Australia 2014.
Song KW, Rifkind J, Al-Beirouti B, Yee K, McCrae J, Messner HA, et al. Subdural hematomas during CML therapy with imatinib mesylate. Leukemia & lymphoma. 2004;45(8):1633-6.
Wei Y, Hardling M, Olsson B, Hezaveh R, Ricksten A, Stockelberg D, et al. Not all imatinib resistance in CML are BCR-ABL kinase domain mutations. Annals of Hematology. 2006;85(12):841-7.
le Coutre P TE, Varella-Garcia M, et al. Induction of resistance to the Abelson inhibitor STI571 in human leukemic cells through gene amplification. Blood 2000;95(2):1758-66.
Gorre ME, Mohammed M, Ellwood K, Hsu N, Paquette R, Rao PN, et al. Clinical resistance to STI-571 cancer therapy caused by BCR-ABL gene mutation or amplification. Science. 2001;293(5531):876-80.
Elias MH, Baba AA, Azlan H, Rosline H, Sim GA, Padmini M, et al. BCR-ABL kinase domain mutations, including 2 novel mutations in imatinib resistant Malaysian chronic myeloid leukemia patients-Frequency and clinical outcome. Leukemia research. 2014;38(4):454-9.
Yun SM, Jung KH, Kim SJ, Fang Z, Son MK, Yan HH, et al. HS-438, a new inhibitor of imatinib-resistant BCR-ABL T315I mutation in chronic myeloid leukemia. Cancer letters. 2014;348(1-2):50-60.
Wylie A, Schoepfer J, Berellini G, Cai H, Caravatti G, Cotesta S, et al. ABL001, a potent allosteric inhibitor of BCR-ABL, prevents emergence of resistant disease when administered in combination with Nilotinib in an in vivo murine model of chronic myeloid leukemia. Blood. 2014;124(21):398.
Valent P. Imatinib-resistant chronic myeloid leukemia (CML): current concepts on pathogenesis and new emerging pharmacologic approaches. Biologics. 2007;1(4):433-48.
Ursan ID, Jiang R, Pickard EM, Lee TA, Ng D, Pickard AS. Emergence of BCR-ABL kinase domain mutations associated with newly diagnosed chronic myeloid leukemia: a meta-analysis of clinical trials of tyrosine kinase inhibitors. J Manag Care Spec Pharm. 2015;21(2):114-22.
Qin Y, Chen S, Jiang B, Jiang Q, Jiang H, Li J, et al. Characteristics of BCR-ABL kinase domain point mutations in Chinese imatinib-resistant chronic myeloid leukemia patients. Annals of hematology. 2011;90(1):47-52.
Carella AM, Garuti A, Cirmena G, Catania G, Rocco I, Palermo C, et al. Kinase domain mutations of BCR-ABL identified at diagnosis before imatinib-based therapy are associated with progression in patients with high Sokal risk chronic phase chronic myeloid leukemia. Leukemia & lymphoma. 2010;51(2):275-8.
Pfeifer H, Wassmann B, Pavlova A, Wunderle L, Oldenburg J, Binckebanck A, et al. Kinase domain mutations of BCR-ABL frequently precede imatinib-based therapy and give rise to relapse in patients with de novo Philadelphia-positive acute lymphoblastic leukemia (Ph+ ALL). Blood. 2007;110(2):727-34.
Gruber FX, Lundan T, Goll R, Silye A, Mikkola I, Rekvig OP, et al. BCR-ABL isoforms associated with intrinsic or acquired resistance to imatinib: more heterogeneous than just ABL kinase domain point mutations? Medical oncology. 2012;29(1):219-26.
Willis SG, Lange T, Demehri S, Otto S, Crossman L, Niederwieser D, et al. High-sensitivity detection of BCR-ABL kinase domain mutations in imatinib-naive patients: correlation with clonal cytogenetic evolution but not response to therapy. Blood. 2005;106(6):2128-37.
Skorski T. BCR/ABL regulates response to DNA damage: the role in resistance to genotoxic treatment and in genomic instability. Oncogene. 2002;21(56):8591-604.
Sallmyr A, Fan J, Rassool FV. Genomic instability in myeloid malignancies: increased reactive oxygen species (ROS), DNA double strand breaks (DSBs) and error-prone repair. Cancer letters. 2008;270(1):1-9.
Nicolini FE, Corm S, Le QH, Sorel N, Hayette S, Bories D, et al. Mutation status and clinical outcome of 89 imatinib mesylate-resistant chronic myelogenous leukemia patients: a retrospective analysis from the French intergroup of CML (Fi(phi)-LMC GROUP). Leukemia. 2006;20(6):1061-6.
Karimiani EG, Marriage F, Merritt AJ, Burthem J, Byers RJ, Day PJ. Single-cell analysis of K562 cells: an imatinib-resistant subpopulation is adherent and has upregulated expression of BCR-ABL mRNA and protein. Experimental hematology. 2014;42(3):183-91 e5.
Aceves-Luquero CI, Agarwal A, Callejas-Valera JL, Arias-Gonzalez L, Esparis-Ogando A, del Peso Ovalle L, et al. ERK2, but not ERK1, mediates acquired and “de novo” resistance to imatinib mesylate: implication for CML therapy. PloS one. 2009;4(7):e6124.
Hartel N, Klag T, Hanfstein B, Mueller MC, Schenk T, Erben P, et al. Enhanced ABL-inhibitor-induced MAPK-activation in T315I-BCR-ABL-expressing cells: a potential mechanism of altered leukemogenicity. Journal of cancer research and clinical oncology. 2012;138(2):203-12.
Kuroda J, Puthalakath H, Cragg MS, Kelly PN, Bouillet P, Huang DC, et al. Bim and Bad mediate imatinib-induced killing of Bcr/Abl+ leukemic cells, and resistance due to their loss is overcome by a BH3 mimetic. Proceedings of the National Academy of Sciences of the United States of America. 2006;103(40):14907-12.
Wong SM, Liu FH, Lee YL, Huang HM. MPT0B169, a New Antitubulin Agent, Inhibits Bcr-Abl Expression and Induces Mitochondrion-Mediated Apoptosis in Nonresistant and Imatinib-Resistant Chronic Myeloid Leukemia Cells. PloS one. 2016;11(1):e0148093.
Donato NJ, Wu JY, Stapley J, Gallick G, Lin H, Arlinghaus R, et al. BCR-ABL independence and LYN kinase overexpression in chronic myelogenous leukemia cells selected for resistance to STI571. Blood. 2003;101(2):690-8.
Wu J, Meng F, Kong LY, Peng Z, Ying Y, Bornmann WG, et al. Association between imatinib-resistant BCR-ABL mutation-negative leukemia and persistent activation of LYN kinase. Journal of the National Cancer Institute. 2008;100(13):926-39.
Ptasznik A, Nakata Y, Kalota A, Emerson SG, Gewirtz AM. Short interfering RNA (siRNA) targeting the Lyn kinase induces apoptosis in primary, and drug-resistant, BCR-ABL1(+) leukemia cells. Nature medicine. 2004;10(11):1187-9.
Wu J, Meng F, Lu H, Kong L, Bornmann W, Peng Z, et al. Lyn regulates BCR-ABL and Gab2 tyrosine phosphorylation and c-Cbl protein stability in imatinib-resistant chronic myelogenous leukemia cells. Blood. 2008;111(7):3821-9.
White DL, Saunders VA, Dang P, Engler J, Zannettino ACW, Cambareri AC, et al. OCT-1–mediated influx is a key determinant of the intracellular uptake of imatinib but not nilotinib (AMN107): reduced OCT-1 activity is the cause of low in vitro sensitivity to imatinib. Blood. 2006;108(2):697.
Illmer T, Schaich M, Platzbecker U, Freiberg-Richter J, Oelschlägel U, Bonin Mv, et al. P-glycoprotein-mediated drug efflux is a resistance mechanism of chronic myelogenous leukemia cells to treatment with imatinib mesylate. Leukemia. 2004;18(3):401-8.
Soverini S, Colarossi S, Gnani A, Rosti G, Castagnetti F, Poerio A, et al. Contribution of ABL kinase domain mutations to imatinib resistance in different subsets of Philadelphia-positive patients: by the GIMEMA working party on chronic myeloid leukemia. Clinical cancer research : an official journal of the American Association for Cancer Research. 2006;12(24):7374-9.
Buschbeck M, Hofbauer S, Di Croce L, Keri G, Ullrich A. Abl-kinase-sensitive levels of ERK5 and its intrinsic basal activity contribute to leukaemia cell survival. EMBO reports. 2005;6(1):63-9.
Ozaki K, Kosugi M, Baba N, Fujio K, Sakamoto T, Kimura S, et al. Blockade of the ERK or PI3K-Akt signaling pathway enhances the cytotoxicity of histone deacetylase inhibitors in tumor cells resistant to gefitinib or imatinib. Biochemical and biophysical research communications. 2010;391(4):1610-5.
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide contributing to approximately 600,000 deaths each year with this number on the rise in the developing world. The aetiology of HCC has been well characterised, including chronic hepatitis B and C infection as well as alcoholic cirrhosis. Current screening programs for patients at high risk of developing HCC, including ultrasound and alpha-fetoprotein analysis, are neither sufficiently sensitive nor specific to detect early HCC. This reduces the likelihood of detecting HCC when curative treatment is effective. One genetic marker which has been shown to be associated with HCC carcinogenesis is the p16 INK4a/ARF locus. If further research confirms this mutation as a common step in early hepatocarcinogenesis then this maker could be utilised to screen for early HCC lesions in at risk populations. Further research in this area could facilitate the early diagnosis of HCC, improving the efficacy of treatment.
Introduction
Liver cancer is the sixth most common cancer worldwide and the second largest cause of cancer mortality [1]. It has several subtypes including hepatocellular carcinoma (HCC), bile duct cancer, hepatoblastoma, and various other liver sarcomas and carcinomas [2]. Of those subtypes, HCC is the most common, comprising about 78% of all liver cancers [1,2]. HCC is unequally distributed globally with over 80% of cases occurring in either Sub-Saharan Africa or Eastern Asia; predominantly in China [3,4]. When considering Western countries, there is strong evidence from the United States that the incidence of HCC is rising, with nine cancer registries reporting via the National Cancer Institute that there has been a 41% rise in mortality from primary liver cell cancer and a 70% rise overall in incidence between 1980 and 1995 [5].
A similar rise in HCC incidence and death rates in Australia have also been identified; possibly linked to the increased prevalence of Hepatitis B and Hepatitis C infection in Australia [6,7]. Moreover, there is evidence that HCC incidence rates in Australia may be up to two-fold higher than the rates reported by cancer registries such as the Victorian Cancer Registry [8]. A higher rate of HCC has also been reported in Aboriginal and Torres Strait Islander populations; estimated at 2% and 8% in urban and rural areas, respectively, compared with less than 1% for the total Australian population [9].
The aetiology of HCC is well documented in the literature with high rates linked to both hepatitis B and hepatitis C exposure [9]. Other significant causes that may cause patients to present include alcoholic liver disease, non-alcoholic steatohepatitis as well as hereditary conditions such as haemochromatosis, alpha-1 antitrypsin deficiency, and autoimmune disorders (Figure 1) [10,11]. These conditions result in significant parenchymal loss, increased fibrogenesis and inflammatory signalling resulting in cirrhosis; a condition associated with 70-90% of all detectable HCC cases [10,11].
Figure 1. Aetiology of hepatocellular carcinoma
The natural history of HCC growth begins as small asymptomatic nodules which can often take years to develop depending on the aetiological exposure [5]. Small HCCs at detection have relatively long tumour doubling times with tumours of less than five centimetres associated with a survival of 81-100% at one year, and 17-21% at three years without therapy, which suggests that early diagnosis may allow for a greater intervention window [5].
These features make HCC an insidious and difficult disease to clinically detect and investigate. Patients who develop HCC are usually asymptomatic, mostly displaying symptoms related to their chronic liver disease which can become modified with disease progression [6,12]. Examples of this include signs of decompensation such as ascites, encephalopathy, jaundice, and variceal bleeding [12]. Advanced lesions also can present more conspicuously causing obstructive symptoms such as jaundice, diarrhoea, weight loss, and fatigue [13]. These signs are a result of local tumour invasion and growth inside the liver. However, systemic signs can also occur as a result of metastases which can develop in the lung, portal vein, periportal nodes, bone or brain [13]. As a result of these features, HCC is typically diagnosed late in its course with a median survival following diagnosis of 6 to 20 months, and a five-year survival ranging from 12% in those outside major cities and 17% within major cities in Australia. [13,14].
Screening and detection of HCC
Accordingly, screening programs for HCC in at risk groups, those with chronic liver disease or chronic hepatitis infection, is recommended with specialist review forming part of a 6-12 monthly management plan [15]. These programs involve using alpha-fetoprotein (AFP) and ultrasound to screen for the presence of cancer lesions.
AFP is a widely studied screening test marker for HCC with a level above 400 ng/mL regarded as diagnostic [5]. However, two thirds of HCCs less than 4 cm have AFP levels less than 200 ng/mL and up to 20% of HCCs do not produce AFP even when they are very large [5]. Moreover, there is evidence that fluctuating levels of AFP in patients with cirrhosis might reflect flares of HBV or HIV infection or liver disease exacerbation rather than HCC development [16]. Some studies investigating the clinical utility of AFP have suggested it lacks the sensitivity to be useful, with one study suggesting it rarely assisted in a diagnosis [5,17,18]. As a result of this, it has been suggested that AFP testing alone should only be used if ultrasound is unavailable, with the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver recommending it not be used at all [16,18,20]. This therefore limits the use of AFP as a reliable test to screen for HCC in at risk groups. Due to these limitations, other serum markers which include plasma microRNAs such as miR-122 and miR-192, des-gamma-carboxy prothrombin, AFP isoforms and glypican-3 are currently being investigated and evaluated for future use [19,20].
Another modality that is used in HCC screening is ultrasound. Ultrasound can detect large HCCs with high sensitivity and specificity; however, it is less able to reliably identify smaller lesions, which are required if more effective therapy is to be offered [6,19,20]. Ultrasound has been shown to detect 85-95% of lesions 3-5 cm in diameter, but can only achieve a 60-80% sensitivity of 1 cm lesions [5]. A large meta-analysis investigating this in 2009 found similar results demonstrating that surveillance with ultrasound showed a limited sensitivity (64%) for early HCC detection [19]. Combined use of AFP and ultrasound has been shown to increase detection rates, but had a raised combined false positive rate of 7.5% compared to AFP and ultrasound alone at 5.0% and 2.9% respectively [18]. Despite the limitations of these tests, the Royal Australian College of General Practitioners guidelines suggest that patients with chronic liver disease or chronic hepatitis infection should be considered for 6-12 monthly AFP and ultrasound screening [15]. The Asian Pacific Association for the Study of the Liver also recommends surveillance for HCC with both AFP and ultrasound every 6 months [21].
The importance of early HCC detection cannot be understated. The natural history of early tumours is poorly known as most are treated upon diagnosis; however, surgical resection, tranplantation and ablation offer high rates of complete responses and a potential cure in all patients with early HCC [22]. Advanced course HCC has a survival of less than six months without treatment with prognostic factors for survival including anatomical extension of the tumour, performance status and functional hepatic reserve based on the Child-Pugh Score [22-24]. It is from this that researchers are currently investigating superior screening techniques which can identify tumours earlier and with greater sensitivity and specificty to enable earlier intervention and better treatment outcomes.
Cancer biology as the pathway for a HCC screening test
One approach that is currently being investigated in the medical literature focusses on the biology of HCC hepatocarcinogenesis to develop a sensitive early screening test that can guide and detect treatment before the cancer can extend and spread. Mature hepatocytes have an average lifespan of between 200-400 days and rarely proliferate unless stimulated by acute injury [25]. The observation of normally quiescent hepatocytes and cholangiocytes proliferating after partial hepatectomy has highlighted the significant regenerative ability of the liver after acute insult [26]. If this regenerative capacity is compromised, the liver has liver progenitor cells (LPCs) which can expand and regenerate the chronically damaged liver [27,28]. LPCs can propagate and differentiate into two types of liver epithelial cells; hepatocytes and cholangiocytes [27]. These cells have been defined as stem cells because they are clonogenic, with a high growth potential and are able to be induced to differentiate into both types of liver cells and have shown capability in repopulating the liver on transplantation [27-30].
The proliferation and differentiation of LPCs into hepatocytes render them a target population for hepatocarcinogenesis [30]. LPCs have been traced to hepatocytes and are markedly elevated in chronic liver disease [28]. Recent laboratory experimentation has shown a link between induced liver damage in mice and the development of HCC, suggesting a tenable link between LPCs and HCC development [31,32]. LPCs have also been documented in chronic human liver pathologies, such as chronic hepatitis C, which is highly associated with hepatocarcinogenesis [29,33-35]. Analysis of premalignant lesions in HCC have also identified the presence of LPCs, with up to 50% of developed HCCs being shown to express markers of progenitor cells including CK7, CK19, OV6 [35-38] These findings have also been found in further studies on both human and mouse liver cells [38,39]. These results suggest a significant link exists between LPCs and HCC carcinogenesis.
From a molecular analysis of HCC progression, it has been shown that hepatocarcinogenesis is a multistep process that is heterogeneous and not well understood [40]. Progressive genetic alterations have been shown to cause a spectrum of cellular changes starting from cell hyperplasia, proliferation to dysplasia and eventually cancer [28,40]. This model is widely accepted and has been applied to many types of cancer, including HCC [28]. Multiple studies have demonstrated that two tumour suppressor pathways are important in controlling cell proliferation including the retinoblastoma protein pathway and the p53 pathway [28,41]. Most human tumours have genetic mutations, deletions, deregulated methylation or alterations in microRNA signalling in their Retinoblastoma and p53 pathways; making these genes likely candidates in the transformation of non-tumourigenic LPCs to tumourigenic LPCs [42-44].
Future HCC screening with the marker p16 INK4a/ARF
One gene involved in the p53 tumour suppressor pathway which may play a crucial role in hepatocarcinogenesis is the INK4a/ARF locus. Studies have identified variable rates of inactivation of the p16 INK4a/ARF gene in HCC with inactivation ranging in the literature from 35-82% of HCCs depending on the aetiology [45-50]. Studies on HCC mouse models have highlighted the important role of INK4a/ARF in tumourigenesis with concomitant loss of p53 and INK4a/ARF accelerating tumourigenesis and the progression to metastatic lung lesions [51-53]. Furthermore, tumours lacking both p53 and INK4a/ARF demonstrated strong migration and invasion capabilities. This was not demonstrated when p53 itself was inactive; suggesting that INK4a/ARF inactivation may be a critical step in HCC development (Figure 2) [52,53]. Significant evidence suggests that INK4a/ARF are important tumour suppressors encoded at 9p21 [9,46,52-54]. Kaneto et al. suggested that the methylation of the INK4a/ARF locus promoter is an early event in hepatocarcinogenesis, making this gene an ideal candidate for further study in the pursuit for an accurate diagnostic tool for HCC [46].
Figure 2. Stages of hepatocellular carcinoma development
The nature of how genes are inactivated in tumourigenesis is biologically complex. The INK4a/ARF gene can be affected by many different forms of inactivation notably mutations, homozygous deletions or gene methylation [54]. Tannapefel et al. showed that of 71 carcinomas examined, 59% showed aberrant methylation of the INK4a gene [54]. Another recent review suggested that as many as 40-70% of HCCs demonstrate an INK4a methylation resulting in the downregulation of protein expression [55]. The pathogenesis of the ARF gene in HCC was not as clear, with studies finding ARF gene methylations in non-cancerous liver tissue as well as low rates of ARF methylation in human HCC samples [54,55]. Despite this, evidence of promotor methylation has arisen from investigations into the cause of INK4a/ARF inactivation in other tumours such as human cutaneous squamous cell carcinoma and colorectal carcinomas [56,57]. These studies provide evidence that the methylation of the INK4a/ARF gene may be an important step in the hepatocarcinogenesis of HCC and therefore could be an effective clinical marker for the identification of HCC development in at risk patients.
Conclusion
While it is clear from this review that further research needs to be conducted to better understand the role of the INK4a/ARF gene locus in HCC development, the potential for a clincial application remains a potent driver for further research in this area of molecular medicine. While the current screening methods using AFP and ultrasound are considered to be clincially useful in detecting HCC, there exists a space for more accurate modalities to detect early HCC lesions. If future research shows that the INK4a/ARF gene is a common early mutation in HCC hepatocarcinogenesis, then future tests may be developed which can sample high probability sites in the liver or the blood to investigate for DNA which contains this mutation. This could potentially improve the prognosis of patients with HCC development and allow early directed treatment with the possibility of cure.
Acknowledgements
Thank you to Professor George Yeoh for his assistance in proofreading this article and providing support and advice.
Conflicts of interest
None declared.
References
[1] Laursen L. A preventable cancer. Nature. 2014;516(7529):S2-3.
[2] Australian Government. Liver cancer. Australia: Cancer Australia; 2014 [cited 2016 April]. Available from: http://canceraustralia.gov.au/affected-cancer/cancer-types/liver-cancer
[4] Han ZG. Functional genomic studies: insights into the pathogenesis of liver cancer. Annu Rev Genomics Hum Genet. 2012; 9c;13:171-205.
[5] Ryder SD. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (HCC) in adults. Gut. 2003;S3:iii1-iii8.
[6] Law MG, Roberts SK, Dore GJ, Kaldor JM. Primary hepatocellular carcinoma in Australia, 1978–1997: increasing incidence and mortality. Med J Aust. 2000;173:403–5.
[7] El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N. Engl. J. Med. 1999;340:745–50.
[8] Hong TP, Fink M, Dev A, Roberts S Nicoll A, Lubel J, Kronborg I, et al. Novel population-based study finding higher than reported hepatocellular carcinoma incidence suggests an updated approach is needed. Hepatology. 2016;63(4):1205-1212.
[9] Cunningham J, Rumbold AR, Zhang X, Condon JR. Incidence, aetiology, and outcomes of cancer in Indigenous peoples in Australia. Lancet Oncology. 2008;9(6):585–95.
[10] Lee YA, Wallace MC, Friedman SL. Pathobiology of liver fibrosis: a translational success story. Gut. 2015;64(5):830-41.
[11] Intrahepatic arteriovenous shunting due to hepatocellular carcinoma and cirrhosis, and its change by transcatheter arterial embolization. AU Sugano S, Miyoshi K, Suzuki T, Kawafune T, Kubota M SO Am J Gastroenterol. 1994;89(2):184.
[12] Schwartz J, Carithers R, Chopra S. Clinical features and diagnosis of primary hepatocellular carcinoma. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed 2016 June.)
[13] Saunders, WB. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the cancer of the liver Italian program (CLIP) investigators. 1998;28(3):751-5.
[14] Refshuage A, Kalisch D. Cancer survival and prevalence in Australia period estimates from 1982 to 2010. Australian Government: Australian Institute of Health and Welfare. 2012 [cited 2016 Sep]. Available from: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737422721
[15] Lusis N. Clinical guidelines: prevention and early detection of liver (hepatocellular) cancer. Royal Australian College of General Practitioners. 2012 [cited 2016 May] Available from: http://www.racgp.org.au/your-practice/guidelines/national-guide/prevention-and-early-detection-of-cancer/prevention-and-early-detection-of-liver-(hepatocellular)-cancer/
[16] Llovet JM, Ducreux M, Lencioni R, Bisceglie AM, Galle PR, Dufour JF, et al. EASL-EORTC Clinical practice guidelines: management of hepatocellular carcinoma. European Association for the study of liver, European Organisation for Research and Treatment of Cancer. Journal of Hepatology. 2012; 56;908-943.
[17] Ebara M, Ohto M, Shinagawa T, Sugiura N, Kimura K, Matsutani S, et al. Natural history of minute hepatocellular carcinoma smaller than three centimeters complicating cirrhosis. A study in 22 patients. 1986;90(2):289-98.
[18] Bruix J, Sherman M. American association for the study of liver diseases: management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020-2.
[19] Singal A, Volk ML, Waljee A, Salgia R, Higgins P, Rogers M, et al. Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Alimentary Pharmacology & Therapeutics. 2009; (30):37–47.
[20] Colombo M, Chopra S. Prevention of hepatocellular carcinoma and recommendations for surveillance in adults with chronic liver disease. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed 2016 June.)
[21] Omata M, Lesmana L Tateishi R, Chen PJ, Lin S, Yoshida H, et al. Asian pacific association for the study of liver consensus recommendations on hepatocellular carcinoma. Hepatology International. 2010;4:439-474.
[22] Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasegawa H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer. 1985;56(4):918-28.
[23] Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003; 37(2):429-42.
[24] Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329-38.
[25] Malato Y, Naqvi S, Schurmann N, Ng R, Wang B, Zape J, et al. Fate tracing of mature hepatocytes in mouse liver homeostasis and regeneration. J Clin Invest. 2011;121(12):4850-60.
[26] Mishra L, Banker T, Murray J, Byers S, Thenappan A, He AR, et al. Liver stem cells and hepatocellular carcinoma. Hepatology. 2009;49(1):318-29.
[27] Miyajima A, Tanaka M, Itoh T. Stem/Progenitor cells in liver development, homeostasis, regeneration and reprogramming. Cell Stem Cell. 2014;14(5):561-574.
[28] Chen C, Wang G. Mechanisms of hepatocellular carcinoma and challenges and opportunities for molecular targeted therapy. World J Hepatol. 2015; 7(15):1964-1970.
[29] Kumar M, Zhao X, Wang XW. Molecular carcinogenesis of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: one step closer to personalized medicine? Cell Biosci. 2011;1(1):5.
[30] Yamashita T, Wang XW. Cancer stem cells in the development of liver cancer. J Clin Invest. 2013;123(5):1911-8.
[31] Viebahn CS, Benseler V, Holz LE, Elsegood CL, Vo M, Beroloino P, et al. Invadin macrophages play a major role in liver progenitor cell response to chronic liver injury. J Hepatol. 2010;53(3):500-507.
[32] Passman A, Strauss R, McSpadden S, Finch-Edmondson M, Woo K, Diepeveen L, et al. A modified choline-deficient, ethionine-supplemented diet reduces morbidity and retains a liver progenitor cell response in mice. Dis Model Mech. 2015;8(12):1635-41.
[33] Zhang A, London R, Schulz F, Giguère-Simmonds P, Delriviere L, Chandraratana H, et al. Human liver progenitor cell lines are readily established from non-tumorous tissue adjacent to hepatocellular carcinoma. Stem Cells Dev. 2010; 19(8):1277-84.
[34] Davies R, Knight B, Tian Y, Yeoh G, Olynyk J. Hepatic oval cell response to the choline-deficient, ethionine supplemented model of murine liver injury is attenuated by the administration of a cyclo-oxyenase 2 inhibitor. Carcinogenesis. 2006;27(8):1607-1616.
[35] Roskams T. Liver stem cells and their implication in hepatocellular and cholangiocarcinoma. Oncogene. 2006;25(27):3818-22.
[36] Mishra L, Banker T, Murray J, Byers S, Thenappan A, He AR, et al. Liver stem cells and hepatocellular carcinoma. Hepatology. 2009;49(1):318-29.
[37] Roskams T. Liver stem cells and their implication in hepatocellular and cholangiocarcinoma. Oncogene. 2006; 25(27):3818-22.
[38] Li C, Wang Y, Dong W, Xiang S, Liang H, Wang H, et al. Hepatic oval cell lines generate hepatocellular carcinoma following transfection with HBx gene and treatment with aflatoxin B1 in vivo. Cancer Letters. 2011;311(1):1-10.
[39] Mishra L, Banker T, Murray J, Byers S, Thenappan A, He AR, et al. Liver stem cells and hepatocellular carcinoma. Hepatology. 2009;49(1):318-329.
[40] Cha C, Dematteo RP. Molecular mechanisms in hepatocellular carcinoma. Best Pract Red CL GA. 2004;19(1):25-37.
[41] Sherr CJ, McCormick F. The RB and p53 pathways in cancer. Cancer Cell. 2002;2(2):103-112.
[42] Ito T, Nishiada N, Fukuda Y, Nishimura T, Komeda T, Nakao K. Alterations of the p14(ARF) gene and p53 and p53 status in human hepatocellular carcinoma. J Gastroenterol. 2004;39(4):355-361.
[43] Gramantieria L, Fornaria F, Challengaria E, Sabbioni S, Lanza G, Croce CN, et al. MicroRNA involvement in hepatocellular carcinoma. J Cell Mol Med. 2008; 12(6):2189-2204.
[44] Tannapfel A, Busse C, Weinans L, Benicke M, Katalinic A, Geissler F, et al. INK4a-ARF alterations and p53 mutations in hepatocellular carcinomas. Oncogene. 2001;20(48):7104-7109.
[45] Tannapfel A, Wittekind C. Genes involved in hepatocellular carcinoma: deregulation in cell cycling and apoptosis. Virchows Arch. 2002;440(4):345-52.
[46] Kaneto H, Sasaki S, Yamamoto H, Itoh F, Toyota M, Suzuki H, et al. Detection of hypermethylation of the p16(INK4A) gene promoter in chronic hepatitis and cirrhosis associated with hepatitis B or C virus. Gut. 2001;48(3):372-7.
[47] Jin M, Piao Z, Kim NG, Park C, Shin EC, Park JH, et al. p16 is a major inactivation target in hepatocellular carcinoma. Cancer. 2000;89(1):60-8.
[48] Lee S, Lee HJ, Kim JH, Lee HS, Jang JJ, Kang GH. Aberrant CpG island hypermethylation along multistep hepatocarcinogenesis. Am J Pathol. 2003;163(4):1371-8.
[49] Li B, Liu W, Wang L, Li M, Wang J, Huang L, et al. CpG island methylator phenotype associated with tumor recurrence in tumor-node-metastasis stage I hepatocellular carcinoma. Ann Surg Oncol. 2010;17(7):1917-26.
[50] Roncalli M, Bianchi P, Bruni B, Laghi L, Destro A, Di Gioia S, et al. Methylation framework of cell cycle gene inhibitors in cirrhosis and associated hepatocellular carcinoma. Hepatology. 2002;36(2):427-32.
[51] Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006 Sep;6(9):674-87.
[52] Chen YW, Klimstra DS, Mongeau ME, Tatem JL, Boyartchuk V, Lewis BC. Loss of p53 and Ink4a/ARF cooperate in a cell autonomous fashion to induce metastasis of hepatocellular carcinoma cells. Cancer Res. 2008; 67(16):7589-7596.
[53] Chen YW, Paliwal S, Draheim K, Grossman SR. p19ARF inhibits the invasion of hepatocellular carcinoma cells by binding to CtBP. Cancer Res. 2009;68(2):476-482.
[54] Tannapfel A, Busse C, Weinans L, Benicke M, Katalinic A, Geissler F, et al. INK4a-ARF alterations and p53 mutations in hepatocellular carcinomas. Oncogene. 2001;20(48):7104-7109.
[55] Nishida N, Goel A. Genetic and epigenetic signatures in human hepatocellular carcinoma: a systemic review. Curr Genomics. 2011;12(2):130-137.
[56] Brown VL, Harwood CA, Crook T, Cronin JG, Kelsell DP, Proby CM. p16INK4a and p14ARF tumor suppressor genes are commonly inactivated in cutaneous squamous cell carcinoma. J Invest Dermatol. 2004;122:1284-1292.
[57] Esterller M, Tortola S, Toyota M, Capella G, Peinado MA, Baylin SB, et al. Hypermethylation-associated inactivation of p14ARF is independent of p16INK4a methylation and p53 mutational status. Cancer Res. 2000;60:129.
Background: Medicine is an ever evolving field of knowledge, new practice, and research. There are various clinical research methodologies; the clinical researcher may actively collect patient information, or retrospectively obtain patient data from traditional datasets, such as hard-copy patient records. In more recent years, clinical research has seen the emergence of ‘big data’.
Big data are large electronic databases characterized by the four V’s-volume, variety, veracity and velocity. The rise of big data suggests that there are advantages to its use. One advantage of big data is easy accessibility, which allows information to be obtained and analysed in a short period of time. However, there are shortcomings of using big data in clinical research, mainly with regards to sampling bias and validity. Nonetheless, big data are here to stay in today’s digitised age of medicine, and the researcher must consider the appropriate contexts for the use of big data in clinical research.
Aim: The aim of this paper was to define ‘big data’ in medicine and examine its use in clinical research.
Methods: A literature review was conducted on Ovid MEDLINE to identify relevant literature. The PRISMA statement was used to screen and select articles that would be reviewed for the paper.
Conclusion: The future of big data is promising, with the allure of low-cost, immediate, and comprehensive data, but it is important that clinical researchers understand how to utilise these well for research and knowledge translation.
Introduction
The future of medical practice is shaped by the outcomes of today’s clinical research trials. Medicine is an increasingly data-intensive field reliant on clinical research [1]. For decades, the clinical research industry has conducted large amounts of research by either actively collecting patient data or retrieving it from hard-copy patient records [2]. However, recent years have seen the emergence of ‘big data’ as the key source of data for clinical trials and observational clinical research alike [3,4]. Big data algorithms in medicine broadly refer to the aggregation of individual medical datasets into large, electronic databases that are readily available for data analysis in clinical research [3,5]. The rise of big data in clinical research suggests that there are obvious advantages of its use. However, there are also challenges in optimising its use in clinical research due to the risk of bias [6]. The aim of this paper was to define ‘big data’ in medicine and examine its use in clinical research.
Methods
This literature review examined recent literature that focused on the use of big data in clinical research. This included researching its validity, reliability, advantages, and disadvantages. Recent literature was defined as articles published from 2005 until 2016.
A literature search was performed on Ovid MEDLINE using the following query:
(“validity” OR “reliability” OR “advantages” OR “disadvantages”)
AND
(“administrative data” OR “database” OR “big data” OR “electronic health records” OR “electronic medical record” OR “clinical database”)
AND
(“clinical research” OR “healthcare”)
The PRISMA statement was used when selecting articles for this review (Figure 1). A total of 164 publications were identified through the database searches. One additional record was identified through the bibliography of one of the articles retrieved from the database search. The abstracts of these articles were manually reviewed for relevance to the topic, excluding 119 articles. Full-text screening excluded a further 23 articles due to inappropriate topic focus and repetition. This paper subsequently focused on reviewing 23 articles. These articles were primarily original research articles and systematic reviews.
Figure 1. PRIMSA ow diagram demonstra ng search strategy.
What is big data?
Defining big data in a medical context
Big data in medicine is characterised by the four V’s – volume, variety, veracity, and velocity [7]:
Volume refers to the large amounts of patient information being collected over time and stored, as suggested by the term ‘big data’. Various elements incorporated into big data include patient demographics, history, investigations, diagnoses, and length of stay [8]. Big data are available in the form of registries and patient databases. Registries gather disease- or population-specific information, while patient databases document patient information throughout the course of an illness [8].
Variety of data can be broadly discussed as structured or unstructured data. Structured data is information that is easily stored, searched, retrieved, edited, and analysed digitally, as in keying in patient ID numbers into electronic medical records to access patient information [7]. In contrast, unstructured data include traditional print records, electronic free text, radiographic films, or survey data collected from patients [9].
Veracity concerns the true representativeness of the data. It refers to the goal of achieving validity and credibility in the data set [7].
Velocity represents the rate at which data is recorded and generated to allow timely retrieval for analysis and decision-making [7].
Advantages of using big data
Accessibility and availability
Big data are readily available [10]. Patient records, such as admission history, investigations, diagnostic results, and medications, are all electronically documented on hospital databases. As these hospital databases are installed on staff computers in the hospital, health professionals working in these hospitals are able to easily access this data for review or, increasingly, for clinical research. The integration of multi-pathway patient records1 in big data provides a convenient, comprehensive pool of information available to researchers [11]. This integration facilitates retrospective cohort studies and therefore aids researchers to identify patterns in disease progression and compare the effectiveness of treatments [11].
Cost- and time-efficiency
Given the convenience of data collection using electronic patient registers, the process of obtaining information needed for clinical research is shortened, in comparison to the more time-consuming alternative of manually collecting patient data [12]. Big data are useful in minimising logistical impediments in prospective and retrospective, longitudinal, population-based studies [13,14]. Researchers who require large sample sizes can also easily extract information from the available pool of data in these databases, potentially increasing the study power of their research [13]. The added benefit of being able to use computerised techniques to analyse unstructured data within big data also means that finer data acquisition can be performed, compared to data acquired by laborious, manual extraction from traditional datasets [14]. In addition, this information is available at a low cost, if not free, to clinical research staff, bypassing potential additional costs that might be incurred through manual data collection [15].
Challenges of Big Data
Kaplan et al. [16] suggests that several biases can arise when analysing big data, including, but not limited to, sampling bias and lack of scope in the information recorded. Secondly, the validity of big data is highly dependent on the context in which it is being used [17]. Lastly, minor data security issues may arise from the utilisation of big data.
Sampling bias and lack of scope
Sampling bias of big data can be discussed in terms of its standardisation and completeness. Completeness of data encompasses both its comprehensiveness and whether it is a good representation of the population of interest [17]. Clinical research often requires data collection from a large sample size of patients. As every patient will have different investigations, diagnoses, and treatment plans, every patient will have varying types and amounts of clinical documentation and to differing degrees of detail. There will, therefore, be difficulty in standardising a method for data collection across an array of available patient information to ensure completeness of the data. It is crucial to ensure that the data is complete, otherwise the research results could be subject to information bias [8]. Typically, the ideal method to achieve this is to conduct prospective data collection, minimising omissions [8]. However, as big data is retrospective, it is often difficult to agree upon a decision regarding inclusion of the data or methods to retrieve missing data when medical records are not available [8]. In those situations, the clinical researcher will be required to design algorithms to clean and correct the available data, however it is difficult to design an objective method to validate certain choices made in this process of data collection.
In addition, the coding of information is very much skewed towards documenting and following up the primary diagnoses [17]. As such, secondary diagnoses are often missed or poorly recorded, resulting in a lack of well-documented secondary patient information, such as co-morbidities.
Validity of big data
Joppe defines validity in quantitative research as a criterion that determines whether a research truly measures what it was initially intended to measure [18]. The validity of big data varies between different clinical specialties and the circumstances in which the data is being used [17].
Occasionally, big data may contain incomplete data sets, or even incorrect data, due to errors in transcription or abstraction [8]. There have been instances when data is misclassified during the recording of data during the data coding process [17]. These may occur when a patient undergoes a procedure that treats more than one condition, or in recording a patient’s hospital admission based on presenting complaint [17]. These systematic errors are hence potentially misrepresentative of the data [17]. A literature review by Talbert and Lou Sole [8] in 2013 found that there has been substantial research suggesting that administrative databases, a subset of big data, have only moderate sensitivities and specificities for correct data coding and may underreport procedures [8].
The increasing trend of activity-based funding of hospitals in some countries, such as the United States and Australia, may also influence the information recorded in big data at discharge [19]. Activity-based funding is a policy intervention targeted at restructuring incentives across healthcare systems through a fixed funding allocation for each episode of care administered to each patient, regardless of their duration of stay and resources used [19]. Obvious benefits include reduced hospital costs and shorter hospital stays, however, hospitals may misuse the system to increase revenue by up-coding diagnoses, or focusing on profitable patients and procedures [19]. As a result, the diagnoses and procedures included in the discharge coding within big data may misrepresent the actual situation in the hospital.
It is crucial to note that electronic medical records adapted for clinical research serve the purpose of a clinical care record and are not designed for research [20]. Electronic inpatient databases document the clinician’s case notes, which often focus on treating the patient’s current illness and respond to the individual clinician’s concerns. These may not always correspond with the aims of future clinical researchers. As such, the available information on the patient may not necessarily be as comprehensive as required by the clinical researcher [12].
Analysis of inaccurate data may cause incorrect conclusions to be drawn. In situations where researchers simply use whatever big data are provided to them, the validity of the clinical research is compromised as the data collected and analysed may not truly reflect the research aims.
Data security
Griebel et al. [1] suggest that users who lack experience in using big data and third party users could potentially pose a threat to data confidentiality. Such circumstances may occur when healthcare providers work with commercial corporations and outsource the information to a commercial cloud [1]. However, mitigation strategies, such as the implementation of high-security data authentication protocols to limit access, can be put in place to ensure data security [1]. Examples of high-security data authentication protocols include advanced firewalls to prevent access by unauthorized users and setting up a digital certificate, which requires the user to identify himself or herself [5]. There are also newer techniques, such as obfuscation, where patient data is stored in an encrypted form and decryption is only allowed through authorised privacy manager software [5].
Choosing appropriate contexts to utilise big data in clinical research
Big data are beneficial to clinical research in providing the following information:
Patient demographics and risk factor profile for disease
Big data are highly applicable in the field of patient profile analytics [2]. Big data can be used to identify relationships between patient demographics and disease or treatment outcomes. By routine monitoring and documentation of patient flow and outcomes, big data allow the incidence and prevalence of diseases, as well as the overall outcome amongst selected patient groups, to be estimated [17]. Furthermore, big data are ideal for developing predictive analytic models based on risk factor profile. As big data capture patient demographics, they help the clinical researcher pinpoint patient risk factors specific to certain diseases, draw links with disease progression and hence, has the potential to be used in developing prediction models [17]. Moreover, risk factors can also be prognostic, and highlight the possibility of a future health outcome [17]. When advanced analytics are applied to these patient profiles and patients at risk of developing specific diseases are identified, there is the opportunity to intervene and provide preventive care to the selected group of patients [2].
Patient treatment outcome
Additionally, by combining both structured and unstructured data across multiple disciplines—medical and surgical clinical data, financial and operational data, and genomic data—to match treatments with outcomes, big data can also predict treatment effectiveness for patients [2]. Collectively, these suggest that big data can be useful in calculating the risks and benefits for various outcomes of both a disease and treatment in different patient groups, hence enabling the clinician to provide more efficient and cost-effective care [2,15].
The future of big data
Improvements in big data organisation and an increasing familiarity with using big data will allow clinical researchers to better utilise the data to their advantage. For instance, researchers are progressively able to model inclusion criteria to obtain relevant data [21]. Up and coming technological infrastructure can be expected to springboard the potential of big data in medicine. For example, cloud computing allows big data to be bigger, better and faster. Cloud computing has the potential to provide researchers with multi-scale data integration tools that will help highlight relationships between discrete data entities [22,23]. Cloud computing will also enable researchers to customise personal networks and virtual servers to increase data security of the electronic resources being used [1].
Beyond clinical practice, there is also potential for big data in other healthcare areas [2]. Big data have the potential to integrate population clinical data sets with genomics data, facilitating pharmaceutical development [2]. There is also a role for big data to play in public health surveillance. Big data can aid in analysing and tracking disease patterns, which is of utmost importance in delivering effective and efficient healthcare responses during disease outbreaks [2].
Conclusion
Big data are a useful and efficient source for obtaining patient information. It offers immediate access to large amounts of patient data with high convenience, low cost and easy accessibility. However, big data may be a poor source for immediate causal inference in data analysis as it lacks randomisation. Yet, there is much potential for big data in clinical research and clinical researchers must improve their utilisation of big data in knowledge translation and data analysis. Appropriate handling of big data through well-designed algorithms and data analysis must be done to overcome its limitations. Nonetheless, with its allure of low-cost, immediate, and comprehensive data, the rise of big data is promising. It is here to stay.
Conflicts of interest
None declared.
Acknowledgements
The author of this paper would like to thank Dr Nora Mutalima (Research Co-ordinator Orthopaedic Services, Dandenong Hospital and Adjunct Research Fellow, Monash University) for her critical review and support.
References
[1] Griebel L, Prokosch H, Köpcke F, Toddenroth D, Christoph J, Leb I et al. A scoping review of cloud computing in healthcare. BMC Med Inform Decis Mak. [Internet]. 2015 March [cited 20 May 2016];15(17):1-16. Available from: https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-015-0145-7
[2] Berger M, Doban V. Big data, advanced analytics and the future of comparative effectiveness research. Journal of Comparative Effectiveness Research. [Internet]. 2014 March [cited 25 May 2016];3(2):167-76. Available from: http://www.futuremedicine.com/doi/abs/10.2217/cer.14.2?journalCode=cer
[3] Ketchersid T. Big Data in Nephrology: friend or foe?. Blood Purif. [Internet]. 2014 January [cited 20 May 2016];36(3-4):160-4. Available from: http://www.karger.com/Article/FullText/356751
[4] McCowan C, Thomson E, Szmigielski C, Kalra D, Sullivan F, Prokosch H, Dugas M et.al. Using electronic health records to support clinical trials: a report on stakeholder engagement for EHR4CR. BioMed Research International. [Internet] 2015 June [cited 2 October 2016];2015:1-8. Available from: http://dx.doi.org/10.1155/2015/707891
[5] Jee K, Kim G. Potentiality of big data in the meidcal sector: focus on how to reshape the healthcare system. Healthcare Informatics Research. [Internet] 2013 June [cited 2 October 2016];19(2):79-85. Available from: https://pdfs.semanticscholar.org/4775/76cda199a58c938423fb4742a89ab429b6d4.pdf
[6] Van Walraven C, Austin P. Administrative database research has unique characteristics that can risk biased results. Journal of Clinical Epidemiology. [Internet]. 2012 February [cited 20 May 2016]; 65 (2): 126-31. Available from: http://www.sciencedirect.com/science/article/pii/S0895435611002484
[7] Raghupathi W, Raghupathi V. Big data analytics in healthcare: promise and potential. Health Inf Sci Syst. [Internet] 2014 February [cited 24 May 2016];2(1):3. Available from: http://hissjournal.biomedcentral.com/articles/10.1186/2047-2501-2-3
[8] Talbert S, Lou Soule M. Too much information. Clinical Nurse Specialist. [Internet] 2013 March [cited 24 May 2016];27(2):73-80. Available from: http://journals.lww.com/cns-journal/Abstract/2013/03000/Too_Much_Information__Research_Issues_Associated.7.aspx
[9] Berger M, Doban V. Big data, advanced analytics and the future of comparative effectiveness research. Journal of Comparative Effectiveness Research. [Internet]. 2014 March [cited 25 May 2016];3(2):167-76. Available from: http://www.futuremedicine.com/doi/abs/10.2217/cer.14.2?journalCode=cer
[10] Jolley, RJ et al. Validity of administrative data in recording sepsis: a systematic review. Critical Care. [Internet]. 2015 April [cited 25 May 2016]; 19(1):139. Available from: https://ccforum.biomedcentral.com/articles/10.1186/s13054-015-0847-3
[11] Sterckx S, Rakic V, Cockbain J, Borry P. “You hoped we would sleep walk into accepting the collection of our data”: controversies surrounding the UK care.data scheme and their wider relevance for biomedical research. Medicine, Health Care and Philosophy. [Internet] 2016 June [cited 25 May 2016];19(2):177-90. Available from: http://link.springer.com/article/10.1007/s11019-015-9661-6
[12] Byrne N, Regan C, Howard L. Administrative registers in psychiatric research: a systematic review of validity studies. Acta Psychiatrica Scandinavica. [Internet] 2005 December [cited 25 May 2016]; 112 (6): 409-14. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1600-0447.2005.00663.x/full
[13] Lopushinsky SR et al. Accuracy of administrative health data for the diagnosis of upper gastrointestinal diseases. Surgical Endoscopy. [Internet] 2007 October [cited 1 June 2016];21(10)1733-7. Available from: http://link.springer.com/article/10.1007/s00464-006-9136-1
[14] Murdoch T, Detsky A. The inevitable application of big data to health care. The Journal of the American Medical Association. [Internet] 2013 April [cited 2 October 2016];300(13):1351-2. Available from: jama.jamanetwork.com/article.aspx?articleid=1674245
[15] Angus D. Fusing randomized trials with big data. JAMA. [Internet] 2015 August [cited 1 June 2016]; 314(8):767-8. Available from: http://jama.jamanetwork.com/article.aspx?articleid=2429723&linkId=16464498
[16] Kaplan R, Chambers D, Glasgow R. Big data and large sample size: a cautionary note on the potential for bias. Clinical and Translational Science.[Internet] 2014 July [cited 1 June 2016]; 7(4):342-6. Available from: http://onlinelibrary.wiley.com/doi/10.1111/cts.12178/full
[17] Cook J, Collins G. The rise of big clinical databases. British Journal of Surgery. [Internet]. 2015 January [cited 20 May 2016];102(2): 93-101. Available from: http://onlinelibrary.wiley.com/doi/10.1002/bjs.9723/full
[18] Joppe, M. The Research Process.[Internet]. Ryerson University. 2000 [cited 3 March 2017]; Available from: http://ryerson.ca/~mjoppe/rp.htm
[19] Palmer K, Agoritsas T, Martin D, Scott T, Mulla S, Miller A et al. Activity-based funding of hospitals and its impact on mortality, readmission, discharge destination, severity of illness, and volume of care: a systematic review and meta-analysis. PLoS ONE. [Internet] 2014 October [cited 1 June 2016];9(10): 1-14. Available from: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0109975
[20] Dean, BB et al. Review: use of electronic medical records for health outcomes research: a literature review. Medical Care Research and Review. [Internet] 2009 December [cited 2 June 2016]; 66(6): 611-38. Available from: http://mcr.sagepub.com/content/66/6/611.short
[21] John P. A. Ioannidis . Informed Consent, Big Data, and the Oxymoron of Research That Is Not Research. The American Journal of Bioethics. [Internet] 2013 March [cited 2 June 2016]; 13(4): 40-2. Available from: http://www.tandfonline.com/doi/abs/10.1080/15265161.2013.768864?journalCode=uajb20 DOI: 10.1080/15265161.2013/768864
[22] Scruggs S, Watson K, Su A, Hermjakob H, Yates J, Lindsey M et al. Harnessing the heart of big data. Circulation Research. [Internet] 2015 March [cited 2 June 2016];116(7):1115-9. Available from: http://circres.ahajournals.org/content/116/7/1115.short
[23] Sessler D. Big Data – and its contributions to peri-operative medicine. Anaesthesia. [Internet] 2013 December [cited 2 June 2016];69(2):100-5. Available from: http://onlinelibrary.wiley.com/doi/10.1111/anae.12537/full
I feel like a dying breed. A dinosaur, if you will. At the outset of my studies I knew this and I still think about it occasionally, still wonder if I made the right decision at the naïve age of 17.
I’m talking of course about my name. Specifically, what’s going to appear after it in just a few years’ time — MBBS. That cultural UK tradition drawn from the fusion of Physicians (Bachelors of Medicine) and Surgeons (Bachelors of Surgery), who at some point decided it was all the same stuff, and that MBBS was more attractive than BM, BS.
In Australia, and in my university, we’re seeing a relatively new kid on the block — the Doctor of Medicine (typically MD). The roots of this seem to come from across the pond, where at some stage Americans decided to silently disagree once again with the conventions of England. In fact, I am the last cohort of MBBS in my university – many of the students below my year boast their superior would-be qualification, and I’ve heard it time and again from universities that already have it. But is MD a new degree, or just a new name? Is this really a new breed of Doc that will one day uniformly scoff at me, a dinosaur from the age of MBBS?
I set about this question in a number of ways. There are the facts and figures, the institutional requirements that fall under the Australian Qualifications Framework (AQF) and the Australian Medical Council. And then there are the perceptions — much more difficult to grasp, but no less important for a degree so public as medicine, where your qualifications guide your job opportunities, your patient trust, and ultimately the ability to help people.
So to the facts. The AQF guides the ability of universities and other tertiary providers to name programs. This is a 10-step ladder, available in an interactive website provided by the AQF [1]. It runs from Level 1 – a Certificate 1, through to Level 10 – a PhD. In Australia, universities are self-accrediting higher education providers, and are overseen by the Tertiary Education Quality and Standards Agency, a Commonwealth Government department. Although I can’t admit to knowing the exact process of application and oversight, the simple fact remains: In Australia, your primary medical degree can be Level 7, Level 8 or Level 9.
Level 7 is a Bachelor degree – there are several broad expectations of someone having attained this level of degree, which is summarised on the AQF website as the following:
“Graduates at this level will have broad and coherent knowledge and skills for professional work and/or further learning” [1].
That seems pretty good to me. Medicine is a profession that I want work in, and I’m very open to further learning – such as a specialty or a research higher degree.
Level 8 is a Bachelor degree with Honours, something provided by many of the universities that still offer MBBS. Although it must be noted that at some universities, Honours is given only to those who undergo extensive research on top of their studies, while at other universities, the requirements seem far less stringent. Level 9 qualification is where MD comes in — according to the AQF levels it is a single Masters degree. The summary of graduates of this level is:
“Graduates at this level will have specialised knowledge and skills for research, and/or professional practice and/or further learning” [1].
This doesn’t seem to mean much to me as a medical student. Surely “specialised knowledge” is gained in postgraduate vocational training, as per the system of Australian Specialist Medical Colleges, in turn overseen by the Confederation of Postgraduate Medical Councils and the AMC [2]? And in terms of research, does that mean I can’t complete useful medical research, with my measly BSc/MBBS?
Maybe the Australian Medical Council could straighten things out for me, and tell me how much I’m worth. The AMC is ultimately responsible for the training of all medical students and doctors in Australia, as dictated by the Medical Board of Australia [3]. This is a huge responsibility – and with medicine changing more and more rapidly over the past 50 years, it’s impressive that they could keep up!
In fact, there is no difference in the AMC accreditation level of university medical graduates. Quite the opposite – the AMC regards all medical students as having had a comparable experience in medical school to make them safe enough for an Australian internship. For the University of Melbourne, the first university to offer the MD in Australia, there was a re-accreditation process with the AMC before the degree could be offered [4]. Likewise, the University of Western Australia overhauled their program, entirely changing the number of years of medical school [5]. But every other medical school in Australia that has switched or is considering switching has not required extensive re-accreditation beyond the normal requirements that exist year-to-year [6][7].
On the ground, what is this meaning for students? Are students becoming better doctors and better scholars, or are they not? My personal feeling is the latter. I have peer-tutored at my university for the year below me, and they do not seem to be a new breed at all. Like me, they wish they started cramming a week earlier with each coming semester. Like me, they whinge when the School makes small program changes that they don’t agree with, or schedules lectures that they think are useless. Like me, they attend Evidence-Based Medicine with a somewhat silent resentment, not because it’s not important but because it’s not exciting.
The School has made some changes; I suppose to be in line with AQF standards. All MD students at my university now write a research protocol – as I understand it, a report on how they might do some research. It’s not revolutionary, it’s not PhD-worthy, and in fact, it’s a lot less than the research required to get an Honours in my current program.
But more than all the facts and figures, I do care about the perceptions. I do wonder if a patient one day will take a look at my name-tag and ask me what an MBBS is, and why they’re not being seen by a real doctor. I wonder if the applications office at RACP or RACS will one day look at my name and think less of me. I wonder if I should have chosen to be the last of the MBBS cohort at my university, or done an extra year of science and slipped into the first MD class. These are worries that can’t easily be put to rest – especially when my juniors already think themselves superior in some way. As though somehow, their research protocol made them able to pick the diagnosis when I would have missed it.
Many students at my university are from overseas, and eventually become fully registered doctors in countries like the US. There, MBBS means nothing, and MD sits in a strange qualifications level that we don’t have in Australia. In many states of America, you can, for a nominal fee, apply to legally change from MBBS to MD after your name, and many of my colleagues will do so [8]. This may be a potential solution to my worries down the track, should they ever really arise.
I decided at the end of the day, that MD is much more about business than health. It was attractive for the University of Melbourne to pioneer a new name, and now each new medical school that “gets the MD” can call themselves on par once again. Unfortunately, the restrictions for Domestic Full-Fee Places in universities do not apply to postgraduate courses such as Masters, which legitimately poses a financial threat to new students, and added strain to the internship crisis [4]. For now, I’m content in the hope that most people don’t care what’s in a name. A medical degree by any other name would doctor just as well. And after all, the Australian National University now provides their students an MChD and nobody seems to complain [9]!
Acknowledgements
The Australian Medical Students’ Association (AMSA) for inviting me to present policy related to this topic.
Conflict of interest declaration
None
References
[1] Australian Qualifications Framework [Internet]. Canberra ACT: Australian Government Department of Education and Training; 2015. AQF Levels; 2013 [cited 2016 Jul 24]. Available from: http://www.aqf.edu.au/aqf/in-detail/aqf-levels/
[2] Confederation of Postgraduate Medical Education Councils [Internet]. Melbourne VIC: Confederation of Postgraduate Medical Education Councils; 2008. Postgraduate Medical Councils; 2008 [cited 2016 Jul 24]. Available from: http://www.cpmec.org.au/Page/about-cpmec-postgraduate-medical-councils
[3] Australian Medical Council Limited [Internet]. Kingston ACT: Australian Medical Council; 2016. About the AMC; 2016 [cited 2016 Jul 24]. Available from: http://www.amc.org.au/about
[4] Roberts-Thomson RL, Kirchner SD, Wong CX. MD: the new MB BS? Med J Aust [Internet]. 2010 Dec [cited 2016 Jul 24];193(11/12):660-661. Available from: https://www.mja.com.au/system/files/issues/193_11_061210/rob11006_fm.pdf
[5] Australian Medical Council [Internet]. Canberra ACT: Medical school accreditation program and status report; 2015 [cited 2016 Jul 24]. Available from: http://www.amc.org.au/accreditation/primary-medical-education/schools/status
[6] Australian Medical Council [Internet]. Canberra ACT: Changes to Primary Qualifications for Admission to Practise Medicine in Australia: Implications for AMC Accreditation; 2012 [updated October 2012; cited 2016 Jul 24]. Available from: http://www.amc.org.au/joomla-fil
[7] University of Queensland [Internet]. Brisbane QLD: Doctor of Medicine (MD); 2016 [cited 2016 Jul 24]. Available from: https://www.uq.edu.au/study/program.html?acad_prog=5578
[8] New York State Education Department Office of the Professions [Internet]. New York NY: New York State Education Department; 2009. Conferral of M.D. Degree; 2009 [updated Dec 15 2009; cited 2016 Jul 24]. Available from: http://www.op.nysed.gov/prof/med/med-mdconferral.htm
[9] Australian Government Department of Industry, Innovation, Climate Change,
Science, Research and Tertiary Education. 2014-16 Mission-based Compact Between The Commonwealth of Australia and The Australian National University. Canberra ACT; 2014 [cited 2016 Jul 24]. 23. Available from: http://docs.education.gov.au/system/files/doc/other/anu_2014-16_compact_final.docx
 He was just about my age, but his face was pale, his cheeks cavernous, and there was a weariness in his every movement; he was too weak to speak or even swallow well. It was as if he had been drained of all his youth.
He was just about my age, but his face was pale, his cheeks cavernous, and there was a weariness in his every movement; he was too weak to speak or even swallow well. It was as if he had been drained of all his youth.