Background: Acquired brain injury (ABI) in childhood can have serious physical, cognitive, and social consequences, although its specific impact on schooling attendance and provision of aid for children is often uncertain. We described educational and neuropsychological outcomes for a population of children with moderate to severe ABI.
Methods: A retrospective cohort study of children with moderate to severe ABI attending a paediatric brain injury service at The Children’s Hospital at Westmead between January 2003 and December 2007 was performed. The children were aged 8-16 at time of injury and information on school attendance, provision of aide, and neuropsychological test results were collected at 6, 18, and 30 months post-injury. Children with previous moderate to severe ABI, neurological disorders or learning difficulties were excluded.
Results: 104 children were included (mean age 12.4, 62.5% male). 48 had severe ABI (Glasgow Coma Scale ≤ 8 or Post Traumatic Amnesia ≥ 7 days). The proportion having returned to full time schooling improved from 56% to 89.7% between the 6 and 30-month follow-up. A majority of children had an impairment recorded on neuropsychological testing. Regression analysis found that severity of injury and language deficit were predictors of attendance in the first six months post-injury. During the 30-month follow-up, 18% of children attended special classes or received a classroom aide.
Conclusion: Time is important in recovery from ABI in children. Neuropsychological deficits influence delivery of classroom aides or modified curricula. Children with severe injury are more likely to have poorer cognitive and educational outcomes.
What is already known about this topic
- Acquired brain injury can lead to serious physical, mental, and social problems for school-aged children
- These deficits can often extend years after the initial injury
- Severity of injury is correlated with poorer outcomes
What this paper adds
- An Australian perspective of educational outcomes for children with moderate to severe brain injury
- Information on deficits experienced by children over two-and-a-half years of follow-up
- A better understanding of the importance of time, neuropsychological deficits, and physical injuries in transition back to school
 Introduction
Introduction
Acquired brain injury (ABI) includes a range of disabilities affecting the brain after birth including traumatic brain injury and haemorrhage. Children with moderate to severe ABI often experience long-term physical, cognitive, or behavioural impairments [1,2]. During discharge planning for these children, families often want to know what to expect from the future. In particular, they worry about the transition from hospital to the home and school environment [3]. Schooling is an important forum for childhood learning, as well as emotional and social development [4]. As such, parents often worry about how and when their children may return to school [5]. These concerns are important to address but are difficult to answer due to the great heterogeneity of outcomes following ABI.
Research has indicated that transition of children with ABI back into school is a challenging time for families. After brain injury, students may need to change their educational and vocational goals to accommodate changes in their abilities [6]. Interviews with children returning to school after ABI raise many issues, including social isolation, missed schoolwork, difficulties adjusting to physical and cognitive changes, and the support provided by schools [7]. Children find it more challenging to participate in school activities than at home and this may be due to the familiarity and greater support provided by the home environment [8].
It has been clearly established by prospective longitudinal studies that severity of injury is associated with poorer physical or cognitive outcomes [1,9-11]. Younger children are also more vulnerable to ongoing consequences of brain injury due to their larger head-to-body ratio, ongoing brain tissue myelination, and their thinner cranial bones [12]. Other factors such as type of injury, socioeconomic status, and provision of family support are also known to affect outcomes following childhood ABI [1,5,7]. Time plays a particularly important role in recovery from ABI however it is useful to note that some deficits may also become more apparent over time.
Neuropsychological testing may also be an early predictor of educational performance and special education requirements: in a study by Kinsella et al., severity of injury and verbal memory and fluency at three months post-injury was a predictor for requirement of special education at 24 months post-injury, Similar findings of the importance of verbal memory influencing educational performance at two years post-injury were made by Catroppa and Anderson as well as Miller and Donders [13,14]. Arnett also found that measures of executive functioning and verbal memory predicted educational competency but did not find these measures predictive of provision of special education [15]. Many studies regarding educational and schooling outcomes for children with ABI do not look specifically at school attendance. Studies of educational outcomes are also limited by small patient numbers and limited follow-up [16].
This study aims to use retrospective data to provide a better understanding of specific neuropsychological and schooling outcomes for children with moderate to severe ABI over a two-and-a-half-year period of follow-up. In particular, the study looks at providing a picture of time for return to schooling and the likelihood of requirement for an aide in the classroom or special education. It also seeks to explore whether neuropsychological factors such as attention, memory, information processing, and executive function, and whether co-morbidities such as fatigue and motor capacity may influence return to school and provision of an aide. This information may enable parents of children with ABI to have a better understanding of what to expect and could improve school engagement in the rehabilitation process [7].
Methods
Participants
Eligible cases were identified from the 2003-2007 database of a paediatric brain injury service at The Children’s Hospital at Westmead, New South Wales, Australia.
Inclusion criteria were age at injury of 8-16 years, moderate or severe ABI, and admission to hospital for ABI. Moderate ABI was defined as Glasgow Coma Scale (GCS) ≤ 12 or Post Traumatic Amnesia (PTA) ≥ 1 day. Severe ABI was defined as GCS ≤ 8 or PTA ≥ 7 days [17]. There were eight cases which were judged as representing moderate or severe ABI but there was unclear GCS and PTA data. These cases were included in order to more accurately represent the patient population and were classified as “undefined” in severity.
Exclusion criteria were previous moderate or severe ABI, previously documented behavioural or developmental difficulties, or previously documented special education support.
Medical records were searched and data extracted from neuropsychological and brain injury clinic reports, discharge summaries, and other hospital records. Data were collected for 0-6, 6-18, and 18-30 months post-injury. Data on educational outcomes of school attendance, provision of classroom aide, and whether children changed school were collected. Data on neuropsychological outcomes was taken from reports written by clinical neuropsychologists at the service. Patient demographics were taken from medical notes. Information on co-morbidities was collected primarily from brain injury clinic reports.
Measures
The neuropsychological testing variables measured were attention, memory, information processing, and executive functioning. Neuropsychological profile was considered intact when reported as “low average” or above. Where terms such as “difficulty”, “reduced”, “borderline”, or “impaired” were used as descriptors in reports they were coded as a deficit. In cases where children had no deficit on initial neuropsychological testing and were subsequently discharged without further testing, it was assumed that they would not develop deficit later on.
This research also collected data on variables concerning other sequelae of ABI including mood/behavior, fatigue, gross and fine motor deficit, receptive and expressive language deficit, visual impairment, and hearing impairment. These deficits were determined by whether they were mentioned as ongoing issues in clinical letters and other medical notes during the set follow-up periods.
Statistical analysis
Quantitative analysis was undertaken using STATA 11 SE. Where possible, variables were coded dichotomously for analysis using Fisher’s Exact Test to look for a relationship with attendance at school or provision of aide. Ordered logistical regression examined which variables (severity, neurological findings, or co-morbidities) were predictive of school attendance.
Ethics approval
Ethics approval was obtained from the Services Improvement Unit at The Children’s Hospital at Westmead, NSW, Australia, approval number: QIE-2011-02-09.
Results
Participant demographics (Table 1)
Of the 158 identified cases, 104 cases met the inclusion criteria. Age at time of injury was between 8-16 years, with the mean age at time of injury being 12.4 years. There were 48 children with severe injury, 48 with moderate injury and 1Table 1.)vehicle accidents. CT/8 with non-traumatic injury, mostly haemorrhage from rupture of arteriovenous malformations. 62.5% were male and three quarters came from urban residencies. 37.5% of injuries were due to falls and 31.7% of children were involved as passengers or pedestrians in motor vehicle accidents. CT and MRI data was collected for 85.6% patients, of which 82% showed abnormalities.
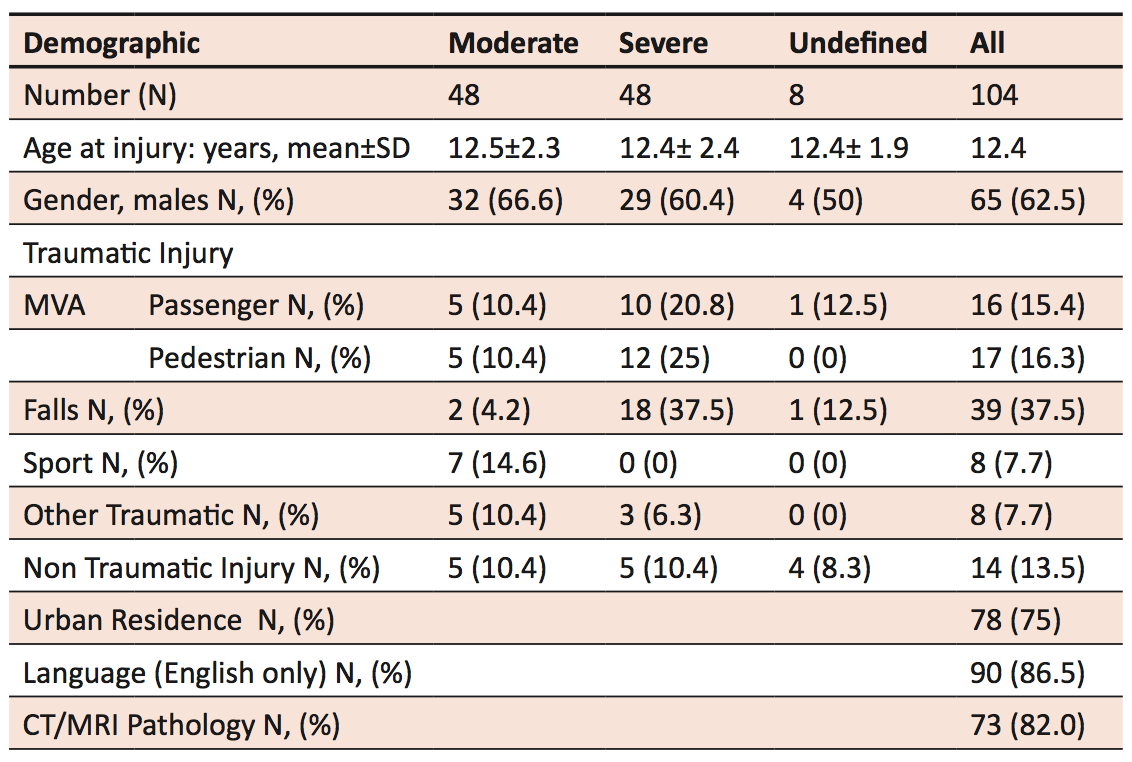
† Note that information is only reported for those cases where it was available.
Undefined cases are cases that were clinically moderate to severe but GCS and PTA were not clearly recorded.
Outcomes
Neuropsychological deficit (Table 2)
Sex and age at onset were not associated with any significant differences in neuropsychological outcomes. As expected, severe ABI has a trend towards more deficits as compared to moderate ABI. Children often had deficits in more than one domain, and children with severe injuries had higher rates of reported deficits. Almost all cases of children who had no deficits on neuropsychological testing were children with moderate ABI. Over time, there was improvement in the numbers of children with reported deficits across attention, memory, information processing, and executive functioning. There was no increase in incidence of deficits over time. Many children with deficits recorded at 0-6 months recovered by 18 or 30 months of follow-up.

Co-morbidities
The most common complaints reported were headache, fatigue, and dizziness. From 0-6 months, 62 children reported fatigue. Mood and behavioural problems were also common, with 61 children reporting problems between 0-6 months, 38 at 6-18 months, and 25 at 18-30 months. Persistence of mood and behavioural problems discussed by parents and children at rehabilitation clinics even two-and-a-half years after injury reflects the ongoing difficulties faced by children with ABI even after physical injuries have healed.
Fine motor deficits were slightly more common than gross motor deficits. For gross motor deficits, from 0-6 months, there were a greater number of children with impaired mobility requiring aid, than those without aide, but between 6-30 months, the majority of children with impaired mobility were able to walk without an aide. Over a fifth of children had initial reports from brain injury clinic reviews describing receptive or expressive language problems, but two thirds of these were resolved by 30 months follow-up. Between 2-8% of children experienced vision or hearing problems after ABI. Except for fine motor deficits, co-morbidities were most frequently recorded during the first 6 months. The frequencies of co-morbidities were recorded at each of the follow-up time points (Table 3).
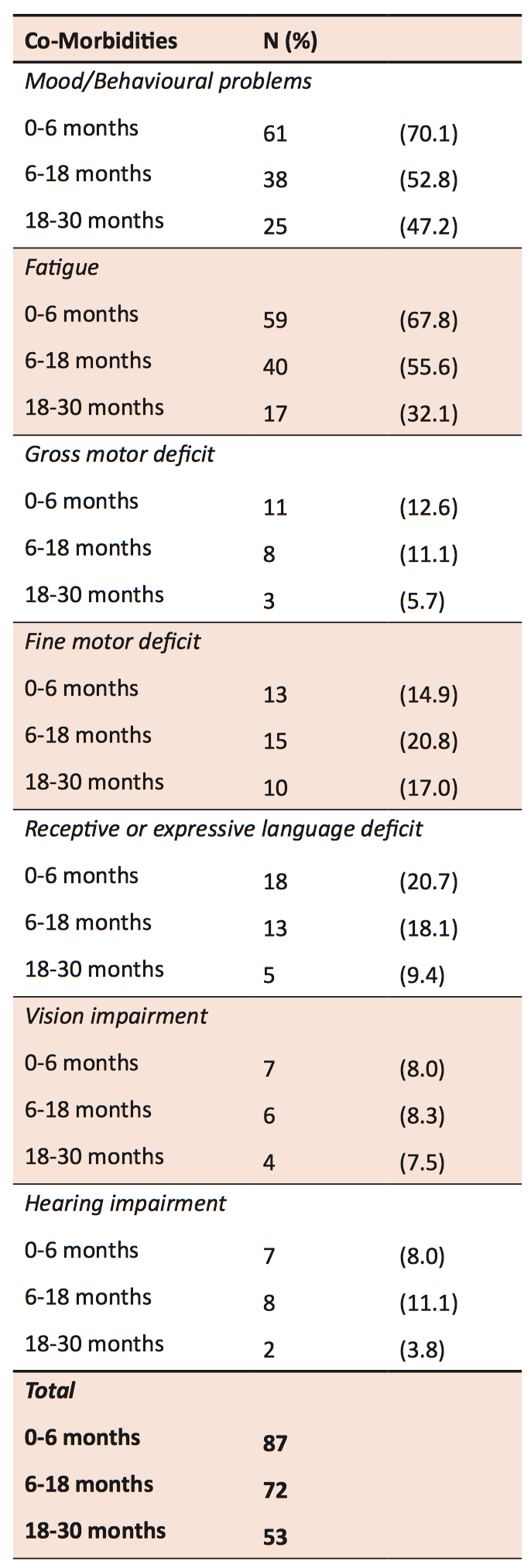
†Note that information is only reported for those cases where it was available for all co-morbidities. This table therefore does not report on the entire sample of 104.
School attendance
Attendance improved over time; most part-time students transitioned into full-time schooling by 18 months (Figure 1). At the end of 18-30 months follow up, 6.9% (n = 87) remained unable to return to full-time schooling.
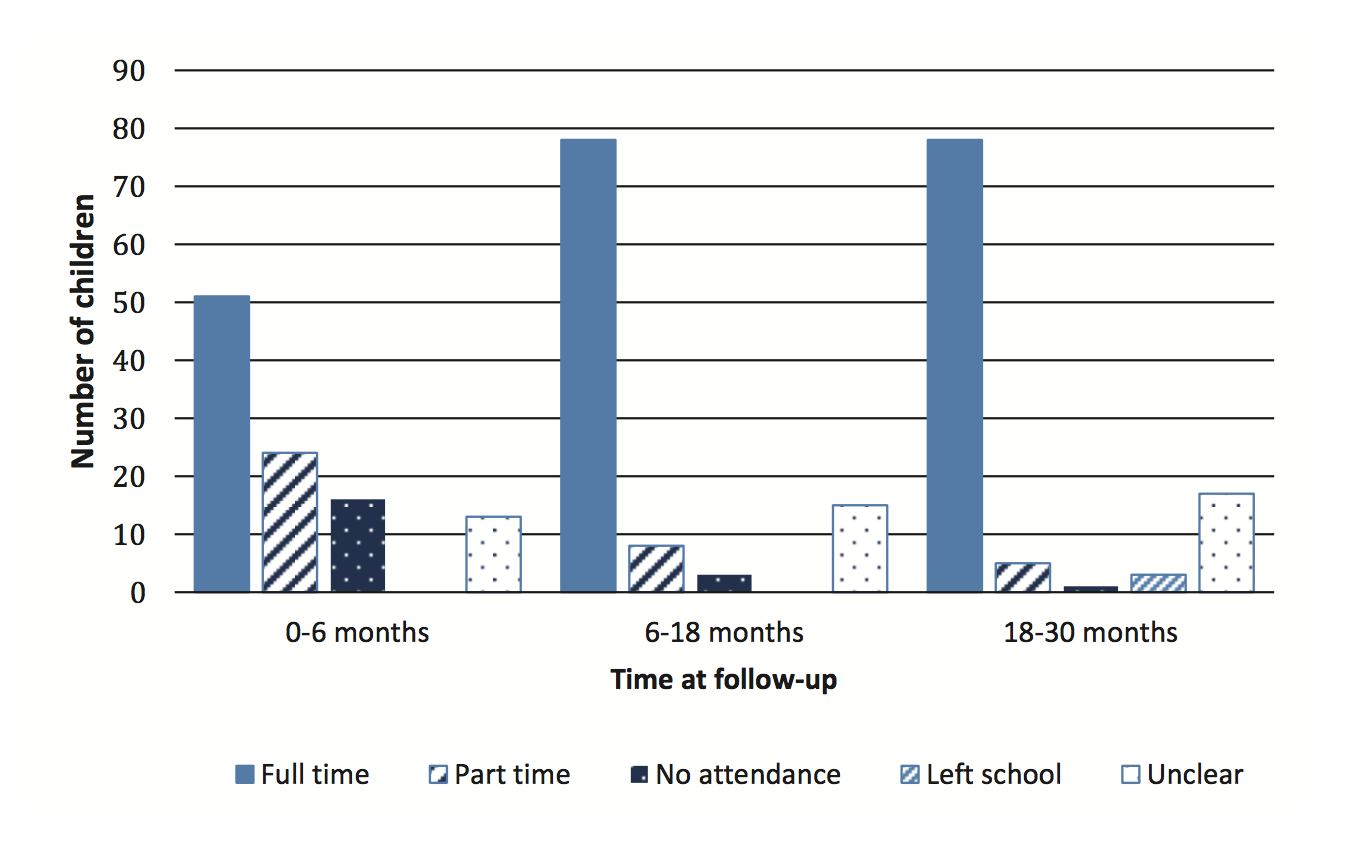
Ordered logistic regression was performed to identify predictors of school attendance. As expected, injury severity was negatively associated with full-time school attendance at 0-6 months post-injury. A child with severe ABI was five times less likely to attend school within six months post-injury than a child with moderate ABI (Table 4). There was a significant difference in school attendance at 18 months post-injury for children with moderate versus severe injury (p < 0.05). No relationship was found at 30 months (p > 0.2). No significant statistical impact of individual neuropsychological measures and attendance of schooling was found.
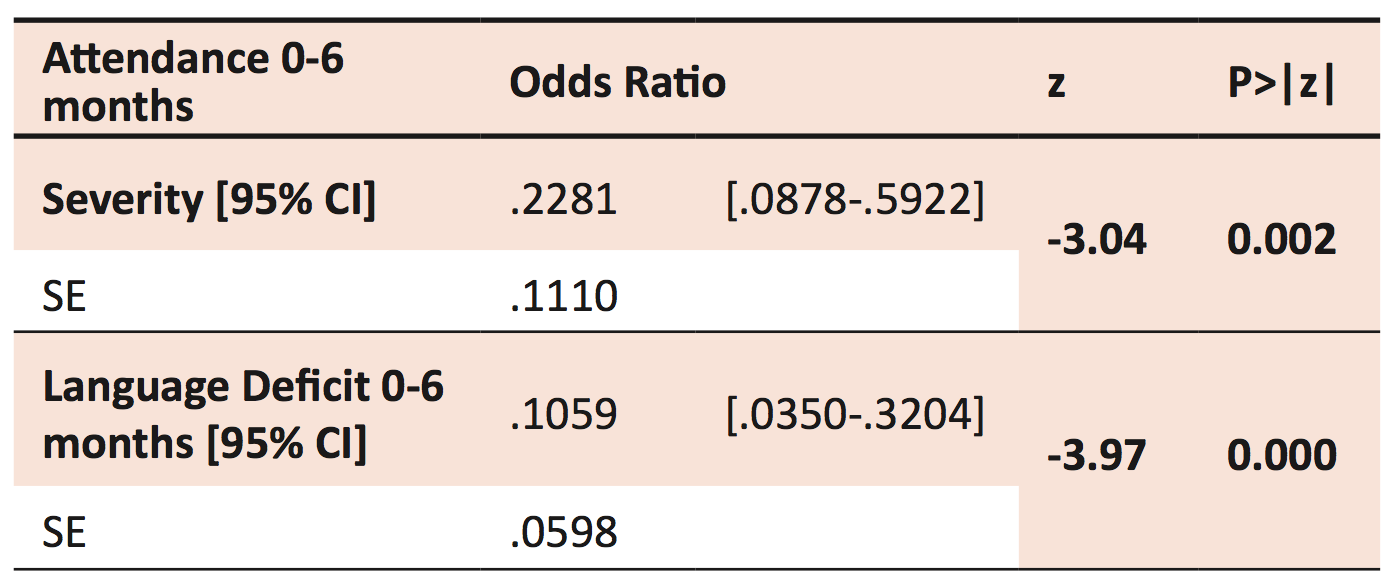
†SE= Standard Error.
Likelihood Ratio chi2(2) = 24.58 Prob > chi2 = 0.0000
Log likelihood = -52.060058 Pseudo R2= 0.191
Of the co-morbidities measured, it was found that injury severity and language deficit (independently and in combination) were negatively associated with full-time school attendance at 0-6 months post-injury. A child with a receptive or expressive language deficit was ten times less likely to attend school within six months post-injury than a child without a known language deficit.
School aide and change of school
Classroom aide was received by 3.3% of children at 0-6 months follow-up, by 12.8% at 6-18 months, and by 13.4% at 18-30 months. There was a significant difference according to injury severity for provision of a teaching aide at 18-30 months (p < 0.03). Special classes or educational programs were provided for 1.1% of children at 0-6 months follow-up, by 5.3% at 6-18 months, and by 7.2% at 18-30 months. There was some overlap with children receiving both aide assistance and attending a special class. During follow-up, seven children required a change of school for reasons relating to their ABI. Of these children, five had experienced severe ABI.
Discussion
This study describes the pattern of children in accessing schooling and special education or aide support following ABI. Extended absences from school are one of the initial challenges facing children after ABI; 17.6% of children in our study population did not attend school in the first six months post-ABI. Whilst hospital and home schooling were sometimes available, this represents a considerable time difference in which children with ABI may fall behind their peers. This study found that a combination of severity of injury and language deficit were found to be predictive of attendance in the first six months after injury. The involvement of language as a predictive factor is important, as it is modifiable. Language is important to complex learning and adaptation and contributes to understanding shared meanings in contexts such as school [18,19]. Language intervention programs may be able to facilitate earlier transition back to school. This study shows that the great majority (93%) of children with moderate or severe ABI will be able to return to full-time schooling. It also shows that the majority of these children are not given provision of classroom aides, special classes, or educational programs.
Attention to classroom instructions, reasoning and expression of ideas, and self-monitoring are all important features of good reintegration to schooling [20]. Children with severe ABI accounted for a greater proportion of neurological deficits in every domain measured (intellect, attention, memory, executive function, and information processing), and 44 of the 45 children with no reported neuropsychological deficits on testing had only moderate ABI. Our study reinforces that there is great variability in the way that ABI affects children, but severe ABI generally has a poorer prognosis and such children may experience greater challenges when returning to school. It is reassuring to note that time can help reduce the burden of ABI, with prevalence of neuropsychological deficits generally improving during follow-up. Longer-term studies suggest that intellect and personality problems may resolve by adulthood, but that reduced quality of life in relation to education and employment can persist [1]. Further long-term follow-up of these patients may be valuable in investigating this. Our study also found that attendance also improves with time, as 89.7% of children were able to resume full-time schooling by 30 months post-injury.
The presence of a classroom aide and modified learning programs is important in exploring whether the ongoing needs of children with ABI are met by schools. Our study found that 13% were provided with classroom aide during 30 months of follow-up. The provision of aid was found to increase over time. This may be accounted for by the inability of children with severe injuries to return to school early but another possible explanation is that there is a delay in the processing and provision of aid.
Quality of aide provision and the satisfaction children and their families had with the schooling system were not measured in this study. This is a possible avenue for future research, as general school educators and also special education teachers often do not have specialised training for working with children with ABI. TBI Consulting Team and BrainSTARS are two promising models currently available for improving professional development of educators in caring for children with ABI, but both require further studies to show objective improvement [21].
In our study, some children reported needing to repeat a year of school. Grade repetition is known to be a de-motivating process that can affect homework completion and predict greater amounts of school absence [22]. A possible direction for future research would be to examine how common grade repetition is amongst the ABI population.
Strengths and limitations of this study
This study addresses the need for a better understanding of educational outcomes for children with moderate to severe ABI. The follow-up time of 30 months also provides a clearer understanding of how outcomes change over time. Additionally, this study deals specifically with school attendance and provision of aide time, two outcomes which are often overlooked in studies describing participation of children in the community following ABI.
The study also provides important information regarding predictors of attendance in the first six months of schooling. Whilst severity has been a known predictor, language has not been a focus for research previously. This new information may help guide health and education professionals in providing appropriate resources to ensure the best educational outcomes for children with ABI [23].
This study had a number of methodical limitations. Due to the highly variable nature of ABI and the small sample size, subgroup analysis was limited. As the study was retrospective there were a number of missing data fields. The results may underestimate true incidence of neuropsychological deficits as standard clinical practice does not comprehensively test children at all points of follow-up if no changes are expected or testing is not necessary. A larger, prospective study of educational outcomes would provide more data for studies with larger patient cohorts to be undertaken in order to confirm our results [24].
The study did not include a control group so confounders were minimised by excluding children with previous intellectual deficits, moderate to severe brain injury, schooling problems, or behavioural difficulties.
This study was unable to detect differences for children who were previously above average, but dropped into an average category on neuropsychological testing. Unfortunately, pre-morbid capabilities are difficult to quantify without formal testing. This study would not consider these children to have a deficit even though they have experienced a change in abilities. Any changes in abilities should not be discounted as they can still negatively impact the expectations and lifestyle of children and their families.
Conclusion
Children with moderate to severe ABI experience a wide range of neuropsychological and physical co-morbidities that can persist for at least 30 months following injury. Greater severity of injury and presence of language deficit are predictive of school attendance of children in the first six months following ABI. 13% of children required additional aide support or involvement in special classes. Over a third of children still reported fatigue and behavioural problems at 30 months follow-up. This study shows that whilst patients and families experience a long and difficult process of recovery, they may be able to expect improvements over time, and children are very likely to have returned to full-time schooling by 30 months post-injury.
Acknowledgements
I would like to thank Dr Angela Morrow for her supervision and guidance throughout this research project. I would further wish to express my gratitude to Dr Barzi for great assistance with the statistics and to Julie-Anne Macey, who came up with the research concept. I would also like to thank Dr Patrina Caldwell for her encouragement and invaluable feedback during the editing process.
References
[1] Anderson V, Brown S, Newitt H, Hoile H. Long-term outcome from childhood traumatic brain injury: intellectual ability, personality, and quality of life. Neuropsychology. 2011;25(2):176-84.
[2] Anderson V, Le Brocque R, Iselin G, Eren S, Dob R et al. Adaptive ability, behavior and quality of life pre and posttraumatic brain injury in childhood. Disabil Rehabil. 2012.
[3] Aitken ME, Mele N, Barrett KW. Recovery of injured children: parent perspectives on family needs. Arch Phys Med Rehab. 2004;85(4):567-73.
[4] Catalano RF, Oesterle S, Fleming CB, Hawkins JD. The importance of bonding to school for healthy development: findings from the social development research group. J School Health. 2004;74(7):252-61.
[5] Beaulieu CL. Rehabilitation and outcome following pediatric traumatic brain injury. The Surgical Clinics of North America. 2002;82(2):393-408.
[6] Stewart-Scott AM, Douglas JM. Educational outcome for secondary and postsecondary students following traumatic brain injury. Brain Injury. 1998;12(4):317-31.
[7] Sharp NL, Bye RA, Llewellyn GM, Cusick A. Fitting back in: adolescents returning to school after severe acquired brain injury. Disabil Rehabil. 2006;28(12):767-78.
[8] Galvin J, Froude EH, McAleer J. Children’s participation in home, school and community life after acquired brain injury. Aust Occup Ther J. 2010;57(2):118-26.
[9] Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Functional plasticity or vulnerability after early brain injury? Pediatrics. 2005;116(6):1374-82.
[10] Anderson VA, Catroppa C, Haritou F, Morse S, Rosenfeld JV. Identifying factors contributing to child and family outcome 30 months after traumatic brain injury in children. J Neurol Neurosur PS. 2005;76(3):401-8.
[11] Catroppa C, Anderson VA, Morse SA, Haritou F, Rosenfeld JV. Outcome and predictors of functional recovery 5 years following pediatric traumatic brain injury (TBI). J Pediatr Psychol. 2008;33(7):707-18.
[12] Catroppa C, Anderson V. Recovery in memory function, and its relationship to academic success, at 24 months following pediatric TBI. Child Neuropsychol. 2007 May; 13(3):240-61.
[13] Miller LJ, Donders J. Prediction of educational outcome after pediatric traumatic brain injury. Rehabil Psychol. 2003;48:237–241
[14] Neuroimaging. 2012;22(2):e1-e17.
Arnett AB, Peterson RL, Kirkwood MW, Taylor HG, Stancin T et al, Behavioral and cognitive predictors of educational outcomes in pediatric traumatic brain injury. J Int Neuropsychol Soc. 2013;19(8):881-9.
[15] Pinto PS, Poretti A, Meoded A, Tekes A, Huisman TA. The unique features of traumatic brain injury in children. Review of the characteristics of the pediatric skull and brain, mechanisms of trauma, patterns of injury, complications and their imaging findings–part 1. J Neuroimaging. 2012;22(2):e1-e17.
[16] Welfare AIoHa. Disability in Australia: trends in prevalence, education, employment and community living. Canberra: AIHW, 2008.
[17] Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81-4.
[18] Marlowe WB. An intervention for children with disorders of executive functions. Dev Neuropsychol. 2000;18(3):445-54.
[19] Ewing-Cobbs L, Barnes M. Linguistic outcomes following traumatic brain injury in children. Semin Pediat Neurol. 2002;9(3):209-17.
[20] Semrud-Clikeman M. Pediatric Traumatic Brain injury: rehabilitation and transition to home and school. Appl Neuropsychol. 2010;17(2):116-22.
[21] Glang A, Todis B, Sublette P, Brown BE, Vaccaro M. Professional development in TBI for educators: the importance of context. J Head Trauma Rehab. 2010;25(6):426-32.
[22] Martin AJ. Holding back and holding behind: grade retention and students’ non-academic and academic outcomes. Brit Educ Res J. 2010;37(5):739-63.
[23] Hawley CA, Ward AB, Magnay AR, Mychalkiw W. Return to school after brain injury. Arch Dis Child. 2004;89(2):136-42.
[24] Slomine B, Locascio G. Cognitive rehabilitation for children with acquired brain injury. Dev Disabil Res Rev. 2009;15(2):133-43.