
Abstract
Background: Excessive and redundant ordering of pathology tests contributes to increasing healthcare costs. Common blood tests, such as full blood counts, liver function tests, serum electrolytes, and C-reactive protein are frequently ordered with little consideration of purpose or intent. Most commonly the ordering of ‘routine’ blood tests is the responsibility of the most junior member of the medical team (the intern). We hypothesise that overutilisation of pathology tests exists due to an under-appreciation of the costs of testing.
Materials and Methods: We surveyed 50 interns regarding their comprehension of the cost of four commonly ordered pathology tests. We also identified the proportion of participants that had ordered an investigation inappropriately.
Results: Full blood counts, serum electrolytes, liver function tests and C-reactive protein were, on average, overestimated in cost by 9%, 32%, 36%, and 71% respectively. Costs for each test were underestimated in only a minority of cases, 32% for full blood counts, 14% for serum electrolytes, 16% for liver function tests, and 18% for C-reactive protein. All participants recall circumstances in which they inappropriately ordered an investigation.
Conclusion: Junior doctors did, on the whole, not underestimate the cost of pathology tests. Junior doctors are poorly informed about the cost of tests, however, this does not appear to influence their ordering, with 100% of participants reporting that they had inappropriately ordered investigations.
Introduction
The use of diagnostic testing is essential in the accurate diagnosis, monitoring, and screening of various diseases [1], with an estimated 70% of clinical decisions being substantially based on the results of such investigations [2]. Over the past 20 years, the number of laboratory tests available to clinicians has more than doubled [3], with most clinical laboratories in Australia reporting a 5-10% increase in their annual workload [4]. Similar to biochemical investigations, the uptake of imaging based diagnostics has growth at a rate of 9% annually [5]. Laboratory medicine is the single highest volume activity in healthcare, with demand increasing disproportionally to other medical activities [6].
Unfortunately, these increased volumes of testing have not always resulted in clinically relevant or useful patient interventions. Indeed, numerous studies [3,7-9] have attempted to investigate the impact of inappropriate pathology testing. While definitions of inappropriate use vary, it can generally be understood as pathology findings that do not have any impact on the clinical decision-making pathway. Estimating the size of this issue is difficult, but has been explored in numerous studies. Miyakis et al [10] found that 68% of a panel of 25 investigations failed to contribute to a patient’s clinical management. Sarkar et al [11] reviewed the cases of 200 patients with haemostatic disorders, and found that 78% of investigations ordered did not influence patient management. This represented an avoidable cost of $200,000. Rogg et al [12] found that repeat investigations are redundantly ordered in 40% of patients transferred from the emergency department to inpatient wards.
Rates of overuse reported in other studies ranged from 40-65%, depending on how ‘appropriate use’ was defined [13-17]. Walraven et al [19] reported, in a systematic review of laboratory clinical audits, pervasive overuse ranging from 4.5-95%. A more recent meta-analysis by Zhi et al [20] estimates the general prevalence of overuse as 20.6%. In Canada, redundant test ordering is expected to represent an annual cost of $36 million (CAD) [21], finances that could have otherwise been redistributed to other essential areas of healthcare.
The impact of inappropriate testing cannot, however, be qualified simply in terms of monetary cost. Even high-value and high-quality investigations can have limitations. False positive results can lead to unnecessary, anxiety provoking, and costly follow-up investigations [22-24]. Appropriate ordering decreases the likelihood of false positive results, thereby reducing the associated physical and emotional stress associated with these false positive values.
Improving the practice of ordering laboratory diagnostics is a challenging issue, the solution of which has been widely studied with variable levels of success. Consensus between these studies seems to suggest that education, audit, and feedback regarding appropriate investigations can limit the demand for diagnostic investigations. Miyakis et al [10] observed a 20% reduction in avoidable testing after education was provided to clinicians regarding their test ordering behaviours, the costs of ordering, and the factors that contributed to overuse. Feldman et al [25] found that attaching fee data to routinely ordered pathology investigations reported an 8.6% reduction in the number of tests ordered. A similar study by Tierney et al [26] reported a 7.7% reduction in the number of tests ordered. Hampers et al [27] found that listing the individual charges of diagnostic tests at the time of ordering resulted in a 27% reduction in the total ordering of diagnostic tests.
Miyakis et al [10] found that junior medical staff are 20% more likely to order unnecessary investigations when compared to senior staff. This observation is vitally important as in public teaching hospitals, junior medical staff are generally most often responsible for the ordering of relevant investigations, often under a degree of self-direction. It is in this group where education regarding cost awareness would be most impactful in reducing inappropriate ordering. Limited numbers of past studies suggest there is a knowledge gap regarding cost comprehension in junior medical staff. Khromona et al [28] found that 82 (70%) respondents at a single institution felt they needed further education into the ordering of appropriate tests. Stanfliet et al [29] found that all interns interviewed (n=61) across two South African Hospitals reported that they would benefit from further education into the appropriate ordering of investigations.
The aim of this pilot study was to evaluate the awareness that junior medical staff (interns) at the Gold Coast University Hospital have of the costs of various commonly requested blood tests. It was hypothesised that systematic over-ordering may be accounted for by underestimation of cost. If this was confirmed, it would be possible to devise educational interventions designed to manage these deficiencies, which may subsequently promote more cost-effective and appropriate investigation. The efficacy of this process has been suggested in previous studies [10,25-27].
Materials and Methods

Study design
The study utilised an observational design, with the development of a questionnaire aimed at assessing cost compression of interns at the Gold Coast University Hospital (Table 1). The questionnaire included questions relating to some of the most commonly ordered investigations at the hospital: full blood count (FBC), liver function tests (LFTs), serum electrolytes (UES), and C-reactive protein (CRP). Additionally, we requested that participants report if they had ever requested a pathology test that they felt was not clinically indicated, or was inappropriate.
Ethics approval to perform this survey was granted by the Human Research and Ethics Committee of the Gold Coast University Hospital (HREC//16/QGC/320).
Participant selection and setting
Medical staff of the classification of intern (first year medical graduates) were approached for inclusion. These staff represented the most junior element of their respective medical/surgical teams. The centre in which this project was conducted is the largest facility of the Gold Coast Health district, which, across its Southport and Robina campuses, serves over 750 beds, with over 100,000 emergency presentations annually. Both campuses are major teaching hospitals, and the majority of interns were graduates of Queensland universities.
The questionnaires were completed during mandatory teaching sessions, which all interns were required to attend. Each participant from the study population had an equal likelihood of being involved in the study. A total of 88 interns were present at these education sessions. Participants were approached randomly with requests for their participation until a sample of 50 participants was reached.
To enhance a response rate and ensure reliability, all surveys were completed during face-to-face meetings with the principal investigator, thus ensuring responders could not have advance understanding of the nature of the specific questions and therefore prepare accordingly by accessing reference materials.
Data collection
The actual cost of the four commonly ordered pathology tests (FBC, CRP, UES, LFTs) according to hospital financial records was used as a comparison with participant estimates. These values are represented as a total dollar value without a breakdown of individual costs, and represent the cost of labour, consumables, processing, and reporting.
Questionnaire responses were de-identified, and no personal or identifying information was retained. Participation and completion of the questionnaire was completely voluntary. This process was repeated until a minimum of 50 completed questionnaires had been collected. It was thought that this number would allow for an equal distribution of uncontrolled variables amongst the study sample.
Statistical analysis
Data was collated using Microsoft Excel 2016 (Microsoft Corporation, Redmond, WA, USA) and statistical analysis was performed using SPSS version 23 (SPSS Inc, Chicago, Ill, USA). Continuous data were analysed for normality using the Kolmogorov-Smirnov method. The mean estimated cost provided by participants was compared to the true cost of the relevant test and was analysed using a one-sample T-test, where p<0.05 was considered statistically significant. Simple graphical representations were used to visualise the number of participants that had overestimated or underestimated the cost of the test. Responses within 25% of the actual cost were regarded as accurate, with estimates more than 25% above the true cost being considered an overestimate, and likewise estimates more than 25% below the true cost being considered underestimates. These thresholds were suggested by a previous systemic review which examined physician cost awareness of pathology testing [29].
Results
A total of 50 interns at the Gold Coast University Hospital were included in this study. The mean assumed cost of pathology testing was, for all tests, higher than that of the true cost.
For almost all tests (with the exception of FBC), costs were routinely overestimated. Costs were overestimated by 50% of participants with respect to UES, 56% of participants with respect to LFTs, and 68% of participants with respect to CRP testing (Figure 1, Table 2). The FBC was the most accurately predicted test, with 40% of respondents accurately estimating the true cost.

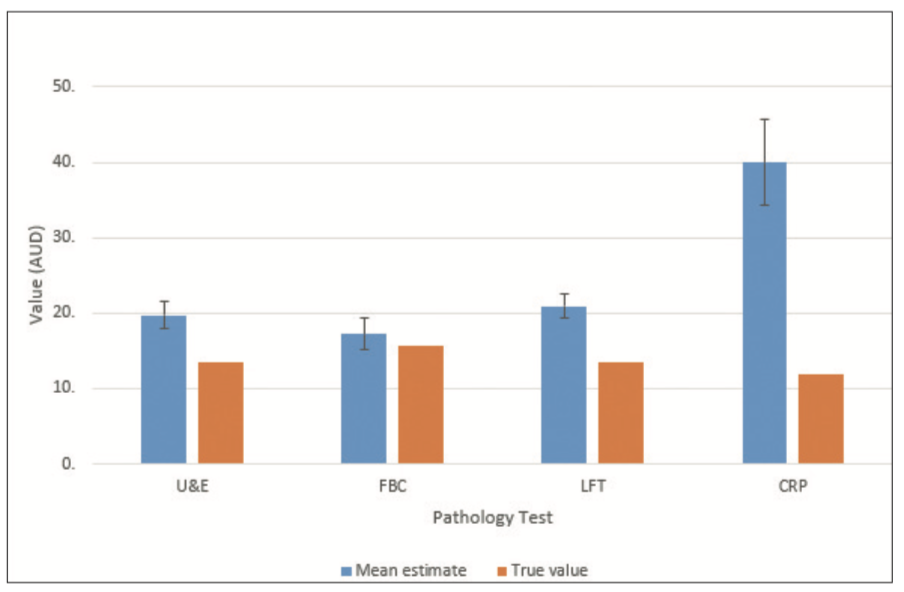
Comparing the mean estimated cost and true value directly, we observed that for LFTs, UES, and CRP testing, there was a statistically significant overestimation of cost. LFTs, UES, and CRP were overestimated by 35.5% ($20.87±10.53, p<0.001), 31.5%, ($19.76±12.55, p=0.001), and 70.6% ($39.97±38.20, p<0.001), respectively when compared to the true costs. FBC testing was overestimated by only 9% ($17.25±13.43, p=0.442).


Of note is that 100% of responders reported ordering an inappropriate pathology test during their clinical practice. We hypothesised this inappropriate ordering would be explained by an assumption that tests were cheaper than their true value; however, this was not the case as the majority of participants were found to overestimate costs for most investigations (Figure 2, Table 3).
100% of participants reported that they had previously ordered tests inappropriately.
Discussion
The results of this study seem to suggest that the understanding of the cost of common pathology tests is highly variable between individuals, with a clear lack of consensus amongst the study group a whole. Surprisingly on average, the estimated cost of pathology testing was generally more than the true cost of testing. In this study 100% of individuals report having ordered a pathology test inappropriately, and various previous studies [7-11] explore the prevalence of test overordering. This would suggest that other factors other than underappreciation of cost are driving excessive ordering amongst medical staff.
It was not surprising that the majority of interns would admit to ordering unnecessary blood tests. This could be because it is often easier to perform the tests with onsite phlebotomy services. Due to the high workload of interns, ordering “routine blood tests” is convenient, time-efficient, and often an expectation of senior staff.
In agreement with previous studies [29,30] interns at the Gold Coast University Hospital demonstrate a poor understanding of the cost of pathology investigations. They also report knowingly ordering inappropriate or unnecessary investigations. We propose three potential explanations for this. First, some participants may have had prior experience with or knowledge of commercial pathology testing, which tends to carry higher costs than in-house hospital pathology tests. Second, due to clinical inexperience, the perceived clinical value of the unnecessary tests was thought to be greater than the monetary costs of performing the investigation. Finally, it is possible that cost reduction is not perceived to be the responsibility of the most junior member of the management team. One study by Tiburt et al [29] in 2013 found that only 36% of physicians considered themselves responsible for reducing healthcare costs. Simply put, many clinicians do not acknowledge or accept their own role in rationalising healthcare costs.
Miyakis et al [10] found that junior staff will order inappropriate investigations 20% more frequently than senior staff (across a single Australian emergency department). However, the same study did not suggest cost-comprehension as a driving force for this difference. Schilling [31] found that only 28% of Swedish emergency department physicians correctly predicted the cost of investigations used to investigate pulmonary emboli, concluding that level of experience did not imply a better knowledge of the costs of investigation. A systematic review by Allan et al [32] of 14 studies of diagnostic and non-drug therapy cost estimates reported that clinicians of various nationalities estimated costs to within 25% of the tests correct value 33% of the time, and that the year of study, level of training, and specialty did not appear to impact this accuracy. These studies were represented by mixed specialties in various European and American based institutions. Broadwater-Hollifeild et al [33] found that only 20% of emergency physicians correctly predicted the costs of common medical tests (within 25% of true cost) across eleven emergency departments in Utah, USA. For comparison as an aggregate, in our study, interns were able to correctly predict cost (within 25% of true value) in 29.5% of proposed tests. The individual populations and settings varied in these studies and the resounding consensus is that clinicians, in general, will poorly predict the cost of investigations.
While experienced clinicians may have a limited knowledge of the costs of the investigations they order, they may request more relevant investigations, likely to be a consequence of experience and a better understanding of the specific indications and limitations of particular tests [33]. However, in some scenarios seniority does not always correlate with a reduced volume of testing. For example, a recent study by Magin et al [34] found that in Australian GPs, for every 6 months of cumulative training, the number of investigations ordered increased by 11%. This indicates the relationship between ordering and experience may be more complex. This may be because with greater comprehension of potential pathology, registrars in later stages of training have greater concern for potential missed diagnoses, or in general have a lower acceptance of ambiguity.
Although unnecessary testing is often associated with a net detrimental effect, examples do exist where excessive ordering of low yield investigations can result in the capture of significant pathology, allowing for the early management of conditions that may have otherwise led to significant mortality and morbidity. These screening programs usually undergo rigorous cost-benefits analyses, ensuring the net benefits outweigh any risks and costs associated with implementing such a program. Some examples of which include routine screening for breast cancer [35] and colorectal cancer [36,37]. These are examples of tests where despite low pretest probability of disease, the impact of a positive value can significantly alter patient mortality and morbidity to the level that routine testing is justifiable for relevant parties. Another example is routine screening for inborn errors of metabolism, which is performed for every child born in Australia. Although these illnesses are rare, these routine tests have high sensitivity and specificity, allowing for early intervention and leading to substantially better outcomes for affected patients [38]. While we acknowledge that this ‘shotgun’ approach can occasionally have positive outcomes, clinicians face an ethical conundrum. Maximising the use of resources in every patient runs the risk of eroding and diluting the overall effectiveness of the healthcare system, and each investigation ordered for a patient increases the risk of a false positive result or adverse event. We do not advocate compromising patient safety in favour of retaining finances, but as 100% of the junior doctors surveyed in this study have ordered inappropriate tests, some degree of cost containment must be considered.
Targeted interventions to curtail unnecessary investigations may assist in this regard. Given the overestimation of costs found in this study, it is unlikely that providing fee data for investigations would impact ordering behaviours significantly. A better approach would be to try and understand what factors are taken into consideration when ordering tests by more senior clinicians, given their tendency to order less inappropriate investigations than interns. Further studies would benefit from comparisons between interns and more senior medical staff, to establish what behaviours in senior staff result in more appropriate test ordering. Targeted education of these concepts may produce a reduction in inappropriate test ordering.
Study limitations and future directions
Our study analysed only awareness of costs, but did not demonstrate or attempt to ascertain the degree of inappropriate usage. Based on our current results we could not provide an opportunity for a cost reduction through education of true cost, as participants generally overestimate rather than underestimate test values.
In future studies, it may be beneficial to include additional questions incorporating a Likert scale in which participants rank the factors most important to them when ordering a blood test (for example, including factors such the cost of the test, expectations from a superior, desire for completeness, and expectations from patients). This would allow for identification of the traits most likely to lead to excessive ordering. Consequently, future interventions could be developed to address factors most likely to contribute to these behaviours. As discussed, it may be beneficial to compare groups of interns to more senior clinicians to establish the behaviours that most strongly correlate with rational test ordering.
Another limitation of this study was that we did not ascertain the degree of previous education regarding pathology testing costs that each participant had received. Previous studies [26,27] suggest that this may be a widespread phenomenon. It would also be valuable to ascertain how many tests participants are ordering to establish if participants who routinely underestimate the cost of tests tend to order more frequently, or vice versa. Such data could be linked to administrative data to assess for clustering and to determine if ordering behaviours vary between departments.
Conclusion
Junior doctors frequently report ordering inappropriate tests and in general, overestimate the costs of these pathology tests. This has a financial impact on the health system. We advocate that pathology services develop educational strategies for reducing inappropriate testing. Cost awareness does not appear to be a highly relevant factor in test ordering. Further study is needed to recognise the specific factors that contribute to systematic over-ordering.
Acknowledgements
I would like to extend my thanks to both Robert Ellis and Miranda Rue-Duffy, who have both been invaluable in providing advice on producing appropriate statistics.
Conflict of interest
None declared.
References
[1] Lippi G, Guidi GC, Plebani M. One hundred years of laboratory testing and patient safety. Clin Chem Lab Med. 2007;45:797-8
[2] Rohr UP, Binder C, Dieterle T, Giusti F, Messina CG, Toerien E, et al. The value of in vitro diagnostic testing in medical practice: a status report. PLoS One. 2016;11:e0149856.
[3] Hickner J, Thompson PJ, Wilkinson T, Epner P, Sheehan M, Pollock AM, et al. Primary care physicians: challenges in ordering in clinical laboratory tests and interpreting results. J Am Board Fam Med. 2014;27:268-74.
[4] National Coalition of Public Pathology. Encouraging quality pathology ordering in Australia’s public hospitals [Internet]. 2011 [cited 2017 Jul]. Available from:
[5] The Royal Australian and New Zealand College of Radiologists. Review of funding for diagnostic imaging services [Internet]. 2011 [cited 2017 Apr]. Available from:
[6] Freedman DB. Towards better test utilisation – strategies to improve physician ordering and their impact on patient outcome. EJIFCC. 2015;26(1):15-30.
[7] Hogg W, Baskerville N, Lemelin J. Cost savings associated with improving appropriate and reducing inappropriate preventive care: cost consequences analysis. BMC Health Serv Res. 2005;5:20.
[8] Hicker JM, Fernald DH, Harris DM, Poon EG, Elder NC, Mold JW. Issues and initiatives in the testing process in primary care physician offices. Jt Comm J Qual Patient Saf. 2005;31:81-9.
[9] Weydert J A, Nobbs N D, Feld R, Kemp JD. A simple, focused, computerized query to detect overutilization of laboratory tests. Arch Pathol Lab Med. 2005;129(9):1141-3
[10] Miyakis S, Karamanof G, Liontos M, Mountokalakis TD. Factors contributing to inappropriate ordering of tests in an academic medical department and the effect of an educational feedback strategy. Postgrad Med J. 2006;82:823-9.
[11] Sarkar MK, Botz CM, Laposata M. An assessment of overutilization and underutilization of laboratory tests by expert physicians in the evaluation of patients for bleeding and thrombotic disorders in clinical context and in real time. Diagnosis. 2017;4(1):21-6.
[13] Rogg JG, Rubin JT, Hansen P, Liu SW. The frequency and cost of redundant laboratory testing for transferred ED patients. Am J Emerg Med. 2013;31(7):1121-3.
[14] Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA. 2012;307(17):1801-2.
[15] Institute of Medicine Roundtable on Evidence-Based Medicine. The National Academies Collection: reports funded by National Institutes of Health. In: Yong PL, Saunders RS, Olsen LA, editors. The healthcare imperative: lowering costs and improving outcomes: workshop series summary. Washington: National Academies Press; 2010.
[16] Bates DW, Boyle DL, Rittenberg E, Kuperman GJ, Ma’Luf N, Menkin V, et al. What proportion of common diagnostic tests appear redundant? Am J Med. 1998;10(4);361-8
[17] Spiegel J S, Shapiro M F, Berman B, Greenfield S. Changing physician test ordering in a university hospital. An intervention of physician participation, explicit criteria, and feedback. Arch Intern Med. 1989;149(3);9549-53.
[18] Schroeder S A, Myers L P, McPhee S J, Showstack JA, Simborg DW, Chapman SA, et al. The failure of physician education as a cost containment strategy. Report of a prospective controlled trial at a university hospital. JAMA. 1984;252(2):225-30.
[19] Van Walraven C, Naylor CD. Do we know what inappropriate laboratory utilization is? A systematic review of laboratory clinical audits. JAMA. 1998;280(6):550-8.
[20] Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962.
[21] Van Walraven C, Raymond M. Population-based study of repeat laboratory testing. Clin Chem. 2003;49:1997-2005.
[22] Moynihan R, Doust J, Henry D. Preventing over diagnosis: how to stop harming the healthy. BMJ. 2012;344:e3502.
[23] Laposata, M. Putting the patient first – using the expertise of laboratory professionals to produce rapid and accurate diagnoses. Lab Med. 2014;45:4-5.
[24] Epner PL, Gans JE, Graber ML. When diagnostic testing leads to harm: new outcomes-based approach for laboratory medicine. BMJ Qual Safe. 2013:22:ii6-10.
[25] Feldman LS, Shihab HM, Thiemann D, Yeh HC, Ardolino M, Mandell S, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;17:903-8.
[26] Tierney WM, Miller ME, McDonald CJ. The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests. N Engl J Med. 1990;322(21):1499-1504.
[27] Hampers LC, Cha S, Gutglass DJ, Krug SE, Binns HJ. The effect of price information on test-ordering behaviour and patient outcomes in a paediatric emergency department. Paediatrics. 1999;103(4 pt 2):877-82.
[28] Khromova V, Gray T. Learning needs in clinical biochemistry for doctors in foundation years. Ann Clin Biochem. 2008;45:33-8.
[29] Tilburt JC, Wynia MK, Sheeler RD, Thorsteinsdottir B, James KM, Egginton JS, et al. Views of US physicians about controlling health care costs. JAMA. 2013;310(4):380-8.
[30] Stanfliet JC, Macauley J, Pillay TS. Quality of teaching in chemical pathology: ability of interns to order and interpret laboratory tests. J Clin Pathol. 2009;62:664-6.
[31] Schilling UM. Cost Awareness among Swedish physicians working at the emergency department. Eur J Emerg Med. 2009;16(3):131-4.
[32] Allan GM, Lexchin J. Physician awareness of diagnostic and nondrug therapeutic costs: a systematic review. Int J Technol Assess Health Care. 2008;24(2):158-65.
[33] Broadwater-Hollifield C, Gren LH, Porucznik CA. Emergency physician knowledge of reimbursement rates associated with emergency medical care. Am J Emerg Med. 2014;32(6):498-506.
[34] Margin PJ, Tapley A, Morgan S. Changes in pathology test ordering by early career general practitioners, a longitudinal study. Med J Aust. 2017;207(2):70-4.
[35] Mackenzie F, Christoph L, Joann E. Breast cancer screening: an evidence-based update. Med Clin North Am. 2015;99(3):451–68.
[36] Beck D. The importance of colorectal cancer screening. Ochsner J. 2012;12(1):7–8.
[37] Lin JS, Piper MA, Perdue LA, Rutter CM, Webber EM, O’Connor E, et al. Screening for colorectal cancer: updated evidence report and systemic review for the US preventative services task force. JAMA. 2016;315(23):2576-94.
[38] Geelhoed EA, Lewis B, Hounsome D, O’Leary P. Economic evaluation of neonatal screening for phenylketonuria and congenital hypothyroidism. J Paediatr Child Health. 2005;41(11):575-9.